




Information
-
HOYT, BRUMM & LINK, INC. 1400 E. Nine Mile Rd. Ferndale, MI 48220-2040 Phone: (248) 548-3355
-
Document No.
-
Name of Injured Employee:
-
Date & Time of Incident:
-
Client / Site
-
HBL Job #:
-
Prepared by
Reporting Requirements
THIS INJURY & ILLNESS INCIDENT REPORT MUST BE FILLED OUT WHENEVER A WORK-RELATED INJURY OR ILLNESS HAS OCCURRED
ATTENTION: Prior to filling out this Incident Report:
-
1. Secure the scene
-
2. Call for emergency services if necessary
-
3. Ensure injured employee gets proper medical treatment
-
4. Contact HBL's Safety Director
-
5. Take Pictures
HBL's Safety Director MUST BE CONTACTED IMMEDIATELY for any:
-
Work-related fatality;
-
Work-related inpatient hospitalization;
-
Amputation;
-
Injury involving the loss of an eye.
Information about the Injured Employee
-
Injured Employee's Name (First, MI, Last):
-
Date of Birth:
-
Last (4) of Social Security #:
-
Sex:
-
Address:
-
Phone Number:
-
Hire Date:
-
Occupation
- Pipefitter / Steamfitter
- Plumber
- Operator
- Shipping & Receiving
- Administrative
- Manager
- Other
-
Journeyman / Apprentice
-
Journeyman / Apprentice
-
How long has injured worker been working in this capacity? (Years / months) (i.e. Welder for 7 yrs. 5 mos).
-
How long has injured worker been working on this project? (Years / months)
-
Date employee attended Contractor's Safety Orientation
-
Date employee attended last safety meeting
-
Does this project require Substance Abuse Testing?
-
Date of employee drug screen
The following information is required for insurance purposes.
-
Tax Filing Status:
-
Number of Dependents:
- 0
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
Information about the Injury
-
-
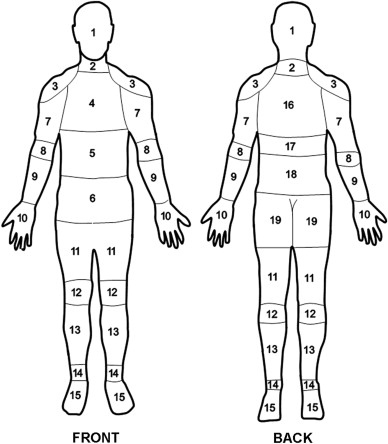
Part(s) of the Body Injured (select all that apply)
- 1 HEAD
- 2 NECK
- 3 SHOULDER
- 4 CHEST
- 5 STOMACH
- 6 ABDOMEN
- 7 UPPER ARM
- 8 ELBOW
- 9 LOWER ARM
- 10 HAND
- 11 HIPS, PELVIS, UPPER LEG
- 12 KNEE
- 13 LOWER LEG
- 14 ANKLE
- 15 FOOT
- 16 UPPER BACK
- 17 MID BACK
- 18 LOWER BACK
- 19 BUTTOCKS, TAILBONE
-
Side
-
Description of Injury (select all that apply)
- Abrasion
- Allergy
- Amputation
- Bruise
- Burn
- Cardiac
- Dermatitis
- Dislocation
- Electric Shock
- Foreign Object in Eye
- Fracture
- Freezing / Frostbite
- Head Injury
- Hearing Loss
- Heat Exhaustion
- Hernia
- Inflammation / Irritatation
- Lacerations (cuts) & Punctures
- Loss of Consciousness
- Poisoning
- Respiratory
- Seizure
- Shock
- Strain / Sprain
- Welding Flash
- Other:
-
Photo(s) of Injury(s) ONLY TAKE PHOTO(S) OF INJURY IF SCENE IS SAFE & SECURE AND INJURED PERSON IS RECEIVING APPROPRIATE MEDICAL CARE. NO PHOTOS OF INJURIES SHALL BE TAKEN THAT INVOLVE SENSITIVE AREAS. CONSENT MUST BE GIVEN BY INJURED PERSON PRIOR TO PHOTO DOCUMENTATION OF INJURED PART!
Information about the Incident
TIMEFRAME
-
What time did the Employee begin work?
-
Did the Employee leave work?
-
What time?
-
Did the Employee return to work?
-
What time?
-
Time of Injury
INFORMATION ABOUT THE INCIDENT
-
Describe specific location of incident on job site.(i.e. column line intersection, building/wing/room name or number, 1st floor, 2nd floor, etc.)
-
If incident happened outdoors, describe conditions (temp., clear, sunny, rain, snow, cloudy, etc.)
-
Cause(s) of Injury(s)
- Fall to: Same Level
- Fall to: Lower Level
- Overexertion: Lifting
- Overexertion: Pulling
- Overexertion: Pushing
- Caught In
- Caught On
- Caught Between
- Struck By: Moving Object
- Struck By: Flying Object
- Struck By: Falling Object
- Struck Against: Stationary Object
- Struck Against: Moving Object
- Struck Against: Protruding Object
- Struck Against: Sharp or Jagged Edge
- Rubbed or Abraded by Friction
- Rubbed or Abraded by Pressure
- Contact with Acid
- Contact with Electricity
- Contact with Toxic Substance
- Contact with Heat
- Contact with Caustic
- Contact with Cold
- Contact with Radiation
- Contact with Noxious Substance
- Other:
-
What was the employee doing just BEFORE the incident occurred? (Describe the activity, as well as the tools, equipment, or material the employee was using. BE SPECIFIC)
-
What happened at the time of injury? (Provide a complete, detailed and accurate description of how the injury occurred)
-
What object(s) or substance(s) directly harmed the employee? (Examples: "concrete floor", "chlorine", "portable band saw". IFTHIS QUESTION DOES NOT APPLY TO THE INCIDENT, LEAVE IT BLANK)
-
Include pictures of the scene / equipment / materials / etc. involved with the incident
WITNESS ACCOUNT(s)
-
Immediate Supervisor's Name & Title
-
Immediate Supervisor's Phone Number
-
Did supervisor actually witness the incident?
-
Supervisor's account of what happened and follow up actions taken
-
Supervisor's Signature
-
Were there any witnesses to the incident?
-
Witness #1 - Name / Company / Trade / Position (i.e. Bob Smith / ABC Company / Pipefitter / Journeymen)
-
Witness #1 - Phone Number
-
Witness #1 account of what happened
-
Witness #1 Signature
-
Are there additional witnesses to the incident?
-
Witness #2 - Name / Company / Trade / Position (i.e. Bob Smith / ABC Company / Pipefitter / Journeymen)
-
Witness #2 - Phone Number
-
Witness #2 account of what happened
-
Witness #2 Signature
Information about the Medical Treatment Provided
-
Medical Treatment Provided
- First Aid
- Sent for Medical Follow-up
- Refused Treatment
- Document Only
-
Name of person that provided first aid
-
General description of first aid provided
-
Name of physician or other health care professional that provided medical treatment
-
Facility Name and Address that provided medical treatment
-
Was injured employee treated in an emergency room?
-
Was the injured employee hospitalized as an in-patient?
-
CALL HBL's SAFETY DIRECTOR DAN GIOVANNANGELI @ (248) 240-6229 IMMEDIATELY!
-
Did the employee suffer an amputation as a result of their injury?
-
CALL HBL's SAFETY DIRECTOR DAN GIOVANNANGELI @ (248) 240-6229 IMMEDIATELY!
-
Did the employee lose an eye as a result of their injury?
-
CALL HBL's SAFETY DIRECTOR DAN GIOVANNANGELI @ (248) 240-6229 IMMEDIATELY!
Post-Incident Substance Abuse Testing
-
Does this facility and/or project require post-incident substance abuse testing?
-
Was post-incident testing performed?
-
Supervisor must provide valid reason why post-incident testing was not performed!
Incident Analysis & Follow-up Evaluation (To be completed by HBL Safety)
ROOT CAUSE ANALYSIS
-
Describe the Contributing Factors (Analyze the suspected cause - get to the Root Cause by asking five (5) why's?
-
Why #1
-
Why #2
-
Why #3
-
Why #4
-
Why #5
IMMEDIATE ACTIONS TAKEN
-
Describe the actions taken immediately following the incident
CORRECTIVE ACTIONS & RECOMMENDATIONS TO PREVENT RE-OCCURENCE
-
Describe the corrective actions and recommendations to be taken to prevent re-occurence
RESTRICTIONS AND ALTERNATE WORK
-
Have restrictions been given?
-
How long?
-
Describe restrictions
-
Is there light duty work available that fits within the medically prescribed restrictions?
-
Describe the type of light-duty work available
Sign-Off
According to Public Law of 1970 (P.L. 91-596) and Michigan Occupational Safety and Health Act 154, P.A. 174, Part 11, Michigan Administrative Rule for Recording and Reporting Of Injuries and Illnesses, this report must be kept on file for five (5) years following the year to which it pertains.
-
Report Completed By:
-
Title:
-
Phone:
