




Information
-
Conducted by
-
Incident Number
-
Date and Time the event occured
-
Time shift started
-
Length of shift
-
Shift
-
Department
- Ancillary
- Contractor
- Dewatering
- Maintenance
- Mill
- Mine
- Ore process
- Security
- Site admin
- Tech Services
-
Which group
- General Store
- Golf Course
- Day Care
- Hadley Maintenance
- Warehouse/Purchasing
- Clinic
-
Which contracting group
-
Which maintenance group
-
Which group
-
Which group
-
Which group
- Accounting
- CI
- Environmental
- HR
- Management
- Safety
-
Which group
- Assay lab
- Projects
- Survey
- Sampling
- Geotech
- Hydrology
- Geology
-
Crew
- Crew 1
- Crew 2
- Crew 3
- Crew 4
- Straight days
- Crew A
- Crew B
- Other (please comment)
-
Is this a High potential incident or High potential near miss
-
At this time does this appear to be a Critical Risk failure
-
Will a MIIT team be used for this investigation
-
Please select all team members
- Employee involved
- Employees peer
- Employees Supervisor
- Dpt. GF or Superintendent
- Employee trainer
- Safety Professional
-
Employees name
-
Peers name
-
Supervisors name
-
GF or Superintendent name
-
Trainers name
-
Safety professional name
Front Line Investigation
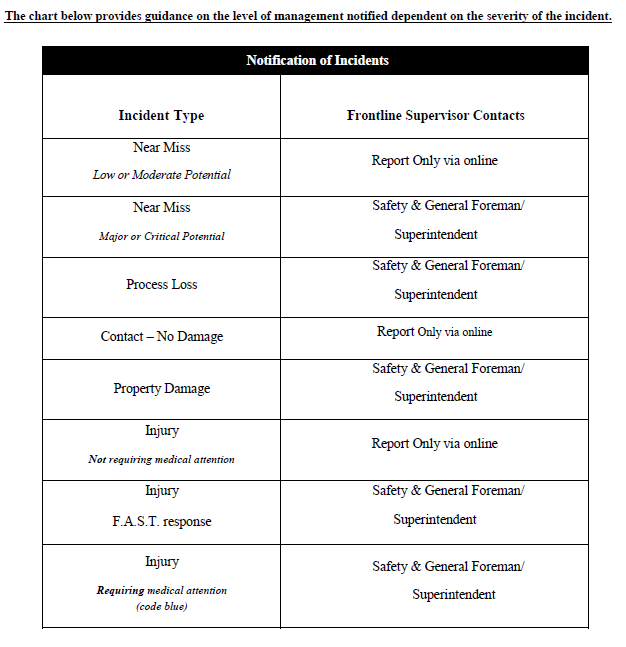
Notification Tree
-
Basic notification tree
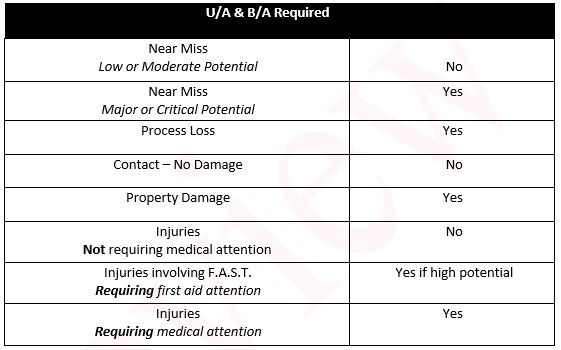
UA/BA determination
-
Select for minimum requirement
- Near miss (low of moderate risk)
- Near miss (major or critical risk)
- Process loss
- Contact-No damage
- Property damage
- Injuries (FAST response)
- Injuries (Requiring medical attention)
-
-
UA/BA conducted
Employee and witness section
-
Are Employees involved
-
Name of Person(s) involved
-
Dept. experience in months
-
RMGC experience in months
-
Total experience with the task
-
Job Title
-
Rotation
- 7 and 7
- 4/5/5/4
- 4 tens
- 8 and 6
- 4/4/4/2
- Other (comment required)
-
Attach employee statment
Witness (add as many as required)
-
Any witnesses?
-
Provide name and job title
-
Upload witness statement(s)
Type of investigation
-
Please select type of investigation for this incident
- Full investigation (MIIT, High potential, CRM, injury)
- Short form (report only/spills)
Investigation Information and Immediate Causes
-
Complete Description of the Incident: Describe where the event occurred, how the event occurred, including events leading up to and following the Incident
-
Incident Type
- Near miss
- Injury
- Contact - No damage
- Property Damage
- Process Loss
- Environmental Impact
- Illness
- Fire
- Atmospheric release
-
Type of Injury
- Abrasion
- Amputation
- Burn
- Contusion
- Fracture
- Foreign Body
- Laceration
- Sprain
- Strain
- Exposure
- Other
-
Affected Body Parts
- Abdomen
- Ankle
- Arm
- Back
- Chest
- Eye
- Finger
- Foot
- Hand
- Head
- Hip
- Knee
- Leg
- Neck
- Shoulder
- Toe
- Wrist
- Respiratory system
- Other (please comment)
-
Attach C-1 form
-
Is the impact cyanide related?
-
Was the reading 10ppm or higher?
-
What was exact reading?
-
Was area/plant evacuated?
-
Was Safety on Call contacted?
-
Please select environmental impact type
-
Attach spill report
-
Attach mortality report
-
Which chemical?
- HCN - Cyanide
- H2S - Hydrogen Sulfide
- Hg - Mercury
- NO2 - Nitrogen Dioxide
- NH3 - Ammonia
- SO2 - Sulfur Dioxide
- Other
-
Was the reading 10ppm or higher?
-
What was exact reading?
-
Was area/plant evacuated?
-
Was Safety on Call contacted?
-
Please select environmental impact type
-
Attach spill report
-
Attach mortality report
-
Physical Activity
- Climbing
- Driving
- Kneeling
- Lifting
- Reaching
- Sitting
- Standing
- Twisting
- Walking
- Other
-
Please describe
-
Work Activity at Time of Incident
- Operating mobile equipment
- Mobile equipment repairs
- Plant operation
- Operating small vehicle
- Passenger
- Facility repairs
- Material handling
- Office Task
- Other (Please comment)
-
Contact or Exposure Type
- Abnormal Operation
- Caught Between/Under
- Caught In
- Caught On
- Environmental Release
- Equipment Failure
- Ergonomic
- Fall - Lower Level/Fall to same level
- Overexertion
- Overpressure
- Overstress
- Struck Against
- Struck By
- No contact near miss
-
Contact Source
- Chemical
- Dust
- Electricity
- Falling Object
- Flying Object
- Heat/Cold
- Loss of Control
- Machinery
- Noise
- Other (please comment)
- Near miss no source
-
Which Chemical?
-
Immediate Causes (normally present at the scene)
- Substandard Acts
- Substandard Conditions
-
Please Select substandard actions
- Failure to Communicate/Coordinate
- Failure to follow SOP
- Failure to Identify Hazard and/or Risk
- Failure to Secure
- Failure to Warn
- Horseplay
- Improper Lifting
- Improper Loading
- Improper Loading
- Improper Placement
- Improper Position for Task
- Improper Use of PPE
- Improper Use of Equipment
- Making Safety Devices Inoperative
- Servicing Equipment in Operation
- Use of Defective Equipment
- Other (please comment)
-
Please select substandard conditions
- Congested/Restricted Area
- Defective Tools/Equipment/Materials
- Fire/Explosive Hazard
- Inadequate Guards/Barriers
- Inadequate Instruction/Procedure
- Inadequate Preparation/Planning
- Inadequate Protective Equipment
- Inadequate Warning System
- Poor Housekeeping/Disorder
- Road Condition
- Weather Condition
- Other (please Comment)
Fatigue Related Incidents
-
What is potentially fatigue related
-
Does the employee believe this event could be due to a medical condition? If so, please stop the assessment and contact the on call HR person
Fatigue Cause
-
To the best of their ability can the employee explain why they are fatigued
- Stress
- Lack of sleep
- Use of medicine
- Grief/Sadness
- Sedentary job/task
- Other (please comment)
Work Schedule
-
Work Schedule
-
How many hours have been worked
- 0-2
- 3-4
- 5-6
- 7-8
- 9-10
- 11-12
- Greater than 12 hours
-
Has the employee taken a break during shift
-
Has the employee taken a break during shift
-
Has the employee taken a break during shift
-
Has the employee taken a break during shift
-
Has the employee taken a break during shift
Signs and Symptoms
-
Physical
- Yawning
- Heavy eyelids
- Rubbing eyes
- head drooping
- None observed
- Other
-
Emotional
- More quiet than usual
- Mood changes, low tolerance or irritability
- Lack of energy
- Emotional outburst, aggression, rage
- None observed
- Other
-
Mental
- Difficulty concentrating on the task
- Difficulty remembering what you are doing
- Failure to communicate important information
- Accidentally doing the wrong thing
- Lapses in attention
- Failure to anticipate events/actions
- None observed
- Other
Sleep Wake History
-
How much sleep have you had in the past 24 hours
- 2
- 3
- 4
- 5
- 6
- 7
- 8
-
How much sleep have you had in the past 48 hours
Scene
-
Photos of scene/damage/area
-
What were the general conditions at the work area
- Congested area
- Slick conditions
- Cluttered (housekeeping)
- Cold/Hot
- Wind
- Clean, orderly, good conditions
- Other (Comments required)
-
Add comments
-
Did the conditions contribute to the incident
-
Please explain
-
Was the incident scene altered prior to investigation (equipment moved etc.)
-
Please describe
-
Was any equipment involved?
-
Equipment Type
-
Manufacturer
-
Model Number
-
RMGC Equipment Number
-
Damage Type
- Mobile Equipment
- Structural
- Machinery
- Small Vehicle
- Utility
- Other
- None
-
Work Order #
-
Estimated Cost of Property Damage and/or Process Loss
-
Work Order #
-
Estimated Cost of Property Damage and/or Process Loss
-
Work Order #
-
Estimated Cost of Property Damage and/or Process Loss
-
Work Order #
-
Estimated Cost of Property Damage and/or Process Loss
-
Work Order #
-
Estimated Cost of Property Damage and/or Process Loss
-
Please specify
-
Work Order #
-
Estimated Cost of Property Damage and/or Process Loss
Corrective Actions and Notifications
-
Description of the Immediate Corrective Actions - Briefly describe what Actions were taken to correct/mitigate the consequences of the event.
-
Complete your portion of the investigation by clicking your department for notification
- Ancillary
- Contractor
- Dewatering
- Environmental
- Maintenance
- Mine
- Mill/OP
- Projects
- Security
- Tech Services
- Administration
Managements investigation Section (HOD)
-
Did an injury or illness occur?
-
Please select the effect of injury/illness
- First Aid
- Medical Treatment
- Restricted Work
- Lost Time
- Fatal
-
What type of care was given?
-
Incident Loss
- Equipment Repair/Replace
- Property Damage
- Production/Process Loss
- Injury/Illness Treatment
- Other (please comment)
-
Estimated Cost
-
Actual Cost
-
Was a work order issued?
-
Work Order#
-
Please describe
-
Estimated Cost
-
Actual Cost
-
Was a work order issued?
-
Work Order#
-
Estimated Cost
-
Actual Cost
-
Was a work order issued?
-
Work Order#
-
Estimated Cost
-
Actual Cost
-
Was a work order issued?
-
Work order#
-
Estimated Cost
-
Actual Cost
-
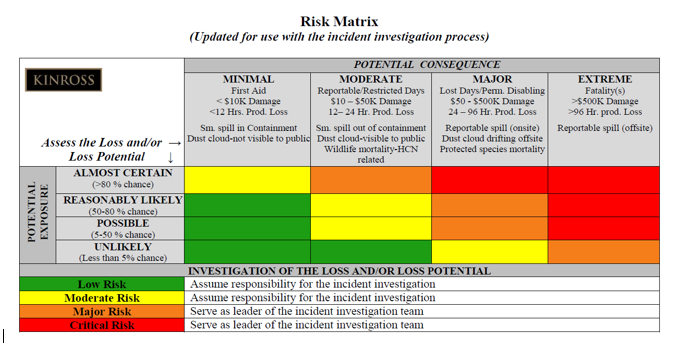
Use the matrix to rank the risk potential
-
Rank the potential risk
-
Basic Cause(s) of Incident (Use appendix C to complete)
- Improper motivation
- Inadequate work standards
- Inadequate leadership and or supervision
- Inadequate communications
- Physical or physiological stress
- Inadequate purchasing
- Inadequate physical/physiological capability
- Mental or psychological stress
- Inadequate engineering
- Inadequate tools and equipment
- Inadequate maintenance
- Lack of skill
- Abuse or Misuse
- Lack of knowledge
- Excessive wear and tear
-
Areas requiring Correction (Use appendix D to complete)
- Leadership and administration
- Emergency Preparedness
- Planned Inspection and Maintenance
- Critical task analysis and procedures
- Incident investigation
- Task Observation
- Standards/Work permits
- Incident analysis
- Knowledge/Skill training
- Personal protective equipment
- health and hygiene control
- System evaluation
- Engineering/change management
- Personal communications
- Group communications
- General promotion
- Hiring and placement
- Materials and service management
- Off the job safety
- Environmental management
- Quality management
-
Was the incident a result of
- Lack of standards
- Inadequate standards
- Non-compliance with standards
Corrective Actions
-
Individual(s) will be assigned to review, revise, develop, manage, coordinate or assume responsibility for the following corrective actions
-
Action Item
-
Assigned to
-
Target Date
-
Completion Date
-
Completion verified by
Final Risk Assessment
-
Will this be classified as a Critical risk failure
-
The Final Risk Assessment is
-
The Risk is
-
Please comment and continue analysis and correction process until final risk is acceptable or practice is abandoned
-
Photos of corrections if possible
Signatures and Approvals
-
Head of Department Signature
-
Head of Health and Safety Department Signature
-
Operations Manager Signature
-
General Manager Signature
-
Complete Description of the Incident: Describe where the event occurred, how the event occurred, including events leading up to and following the Incident
-
Incident Type
- Near miss
- Injury
- Contact - No damage
- Property Damage
- Process Loss
- Environmental Impact
- Illness
- Fire
- Atmospheric release
-
Type of Injury
- Abrasion
- Amputation
- Burn
- Contusion
- Fracture
- Foreign Body
- Laceration
- Sprain
- Strain
- Exposure
- Other
-
Affected Body Parts
- Abdomen
- Ankle
- Arm
- Back
- Chest
- Eye
- Finger
- Foot
- Hand
- Head
- Hip
- Knee
- Leg
- Neck
- Shoulder
- Toe
- Wrist
- Respiratory system
- Other (please comment)
-
Attach C-1 form
-
Description of the Immediate Corrective Actions - Briefly describe what Actions were taken to correct/mitigate the consequences of the event.
-
Send to Incident investigation review team for approval
-
Is the impact cyanide related
-
Please select environmental impact type
COMPLETE SPILL REPORT
-
Date and Time spill occurred
-
Type of material spilled
QUANTITY & CONCENTRATION
-
Is quantity known
-
State quantity
-
Please choose quantity calculation
- Volume of soil/material contaminated equals (ft3)
- Total quantity in Gallons
- Percent of spilled material in soil or percent soil moisture
- Weight of spilled material in the soil in pounds
- If applicable, pounds of cyanide in spilled solution
-
Amount Volume of soil/material
-
Amount in gal
-
Percent of spilled material
-
Weight of spilled material
-
Pounds of cyanide
-
Duration of spill (i.e., 1 minute, 4 hours, two days)
-
Was the material puddled/ponded
-
Exact location on mine site where the spill occurred
-
Do you know the cause of the spill?
-
Please describe and include equipment ID# if applicable.
-
How did you find the spill? Please include equipment ID# if applicable.
-
What type of material was contaminated?
-
Please be specific
-
How was the spill contained?
-
How was it cleaned up?
-
How much contaminated material was removed? (cubic feet or cubic yards)
-
Where was the contaminated material taken?
-
Action taken to prevent re-occurance
FINALIZING SPILL REPORT
-
Date and Time spill clean up was completed
-
Person responsible for spill report
-
Position of person responsible for spill report
-
Supervisor/Manager
-
Attach mortality report
-
Attach C-1
-
Description of the Immediate Corrective Actions - Briefly describe what Actions were taken to correct/mitigate the consequences of the event.
-
Send to Incident investigation review team for approval
-
Which chemical?
- HCN - Cyanide
- H2S - Hydrogen Sulfide
- Hg - Mercury
- NO2 - Nitrogen Dioxide
- NH3 - Ammonia
- SO2 - Sulfur Dioxide
- Other
-
Was the reading 10ppm or higher?
-
What was exact reading?
-
Was area/plant evacuated?
-
Was Safety on Call contacted?
Corrective Actions and Notifications
-
Description of the Immediate Corrective Actions - Briefly describe what Actions were taken to correct/mitigate the consequences of the event.
-
Complete your portion of the investigation by clicking your department for notification
- Ancillary
- Contractor
- Dewatering
- Environmental
- Maintenance
- Mine
- Mill/OP
- Projects
- Security
- Tech Services
- Administration




