




Title Page
-
Jobsite:
-
Insurance Coverage:
-
Claim Number:
-
General Contractor:
-
Project Superintendent:
-
Project Manager:
-
Weather (Take Screenshot from Heat Index App):
-
Contacted Tom Isola @ 407.607.5111
-
Number of Employees:
OSHA'S FORM 301 (Rev. 04/2004)
Attention: This form contains information relating to employee health and must be used in a manner that protects the confidentiality of employees to the extent possible while the information is being used for occupational safety and health purposes.
COMPLETED BY
-
Completed By:
-
Title:
-
Date:
INFORMATION ABOUT THE EMPLOYEE
-
1) First Name:
-
Middle Name:
-
Last Name
-
2) Street:
-
Apt#:
-
City:
-
State:
-
Zip:
-
3) Date of Birth:
-
4) Date of Hire:
-
5) Male of Female:
-
Social Security Number:
-
Employee Number:
INFORMATION ABOUT THE PHYSICIAN OR OTHER HEALTH CARE PROFESSIONAL
-
Medical Attention Required:
-
6) Name of Physician or other Health Care Professional (Located on DWC-25 Bottom Left of Second Page):
-
7) If Treatment was Given Away From the Worksite, Where was it Given:
-
Street:
-
City:
-
State:
-
Zip:
-
Transportation and/or Translation Needed for Future Visits:
-
Work Status:
-
Drug Screen Conducted:
-
THIS IS REQUIRED. CALL TOM ISOLA WITH ANY QUESTIONS
-
8) Was Employee Treated in an Emergency Room:
-
How Was the Employee Transported:
-
9) Was Employee Hospitalized Overnight: as an in-patient:
INFORMATION ABOUT THE CASE:
-
10) Case Number from the Log:
-
(Transfer the case number from the Log after you record the case.)
-
11) Date of Injury or Illness:
-
12) Time Employee Began Work:
-
13) Time of Event:
-
Re fields 14 to 17: Please do not include any personally identifiable information (PII) pertaining toworker(s) involved in the incident (e.g., no names, phone numbers, or Social Security numbers).
-
14) What Was the Employee Doing Just Before the Incident Occurred:
-
Describe the activity, as well as the tools, equipment, or material the employee was using. Be specific. Examples: “climbing a ladder while carrying framing materials”; “spraying form oil from pump can”; “moving material with crane”
-
15) What Happened? Tell us How the Injury Occurred:
-
Examples: "When ladder slipped on concrete slab, worker fell 12 feet”; “Worker was sprayed with form oil in face while spraying forms”; “Finger caught between skip pan and dumpster.”
-
16) What was the Injury or Illness:
-
Examples: “fractured wrist”; “chemical burn, eyes”; “bruised finger.”
-
17) What object or substance directly harmed the Employee:
-
Examples: “concrete slab”; “form oil”; “skip pan” If this question does not apply to the incident, leave it blank.
-
18) If the Employee Died, When did Death Occur:
ROOT CAUSE INVESTIGATION
INJURY DETAILS
-
Injury Cause / Source:
-
Date & Time Incident Reported:
-
Person Reported to:
-
Did the Injury Occur in Course of Employment:
-
Day of the Week:
-
What Part of Employee’s Workday Did the Incident Occur:
-
Was the Employee Working:
-
Pictures of Accident:
BODY INJURIES
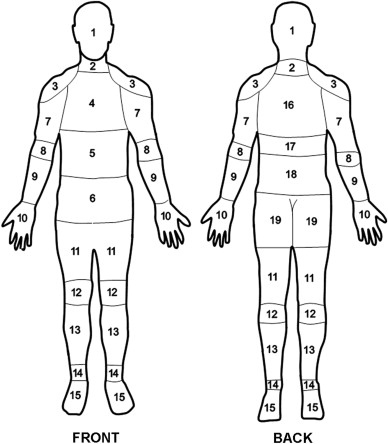
BODY AREA #1
-
Area of Body:
-
Left or Right:
BODY AREA #2
-
Area of Body:
-
Left or Right:
WITNESSES
-
Name & Phone #
-
Name & Phone #
-
Name & Phone #
CORRECTIVE ACTIONS
-
HOW CAN FUTURE INCIDENTS BE PREVENTED?
CONTRIBUTING FACTORS
-
A Root Cause Analysis (RCA) is the process of determining the cause of an incident. It requires consideration of all the factors that may have contributed to this incident occurring and deeply understanding the underlying cause. One tactic to determine this is through asking "Why?" five times, to uncover the core of a problem.
-
Languages Spoken:
-
Occupation:
-
Time in Occupation at Time of Accident:
-
Name of Foreman Responsible:
-
Was the worker following the guidelines to the specific job task?
-
Was a Pre-Task completed for this work procedure?
-
Did the foreman and crew discuss a detailed work plan?
-
Did the work plan address the identified hazard(s)?
-
Were the tools and equipment right for the job?
-
Was the employee capable, trained, and qualified to do this work?
-
Was there enough time to do the task safely?
-
Does the employee normally do this task?
-
Was human factor such as the person’s size or strength a factor?
-
Did the sun, heat, cold, dust, glare, fatigue contribute to the incident?
-
Was the injury a result of the Pre-Task not being followed?
-
Was the worker a new hire (GREEN TAPE) or a transfer (RED TAPE)?
-
Was a Safety Rule of Specific Instruction Violated?
-
Why Did it Happen - Unsafe Acts of People:
-
What were the contributing factors to this incident occurring? (select all that apply):
- Drugs or Alcohol
- Employee Operating at Inappropriate Speed
- Equipment Used Outside Rated Capacity
- Improper Equipment Use
- Inappropriate PPE
- Inadequate Ventilation
- Inadequate Guard
- Lack of PPE
- Not Aware of Surroundings
- No Training or Insufficient
- Personal Issue
- Safety procedures not followed
- Tool or Equipment Defective
- Unauthorized Equipment Use
- Unguarded Hazard
- Unsafe Clothing
- Unsafe Lighting
- Untidy Conditions (Poor Housekeeping)
- Weather Related
-
Has the root cause of this issue been able to be identified?
-
How Likely is This Incident to Reoccur in the Future?
- Certain
- Very Likely
- Likely
- Unlikely
- Very Unlikely
- Never
- Unclear / Not Determinable




")




