Information
-
Site conducted
ATTENTION Prior to filling out this Accident Report: 1. Secure the scene of the accident 2. Provide treatment 3. Call for emergency services if necessary 4. Take pictures of the scene
-
Name of Injured Employee
-
Client / Site
-
Conducted on
-
Prepared by
INSTRUCTIONS
-
1. Provide immediate medical attention if necessary. Call Carl or Payroll immediately to authorize treatment/drug testing. Drug/Alcohol test is required for all employee injuries.
2. Within 8 hours, complete this form and the form: 'Root Cause Analysis (Fishbone)' for all job related injuries AND near misses.
3. Whenever possible, the foreman and the injured employee will sign the form.
INFORMATION ABOUT THE INJURED
-
Name
-
Sex
-
Date of Hire
-
Date of Birth
-
Home Address
-
Phone
-
Social Security Number
-
Job Title
-
What time did the Employee begin work?
-
Did the Employee leave work?
-
What time?
-
Did the Employee return to work?
-
What time?
-
Did you authorize medical treatment?
-
Have restrictions been given?
-
How long?
-
Describe restrictions
-
Is there light duty work available?
-
Fatality?
-
CALL CARL IMMEDIATELY!
-
Were three or more employees injured?
-
CALL CARL IMMEDIATELY!
-
Drug/alcohol test?
-
THIS IS REQUIRED. CALL MAIN OFFICE IF YOU HAVE ANY QUESTIONS.
INFORMATION ABOUT THE ACCIDENT
-
Date and time of the accident
-
Date accident is being reported
-
JOB INFORMATION
-
Location Name
-
Describe specific location of incident on job site
-
Job Number
-
Address
-
Foreman
-
Describe what happened and probable cause of accident
-
-
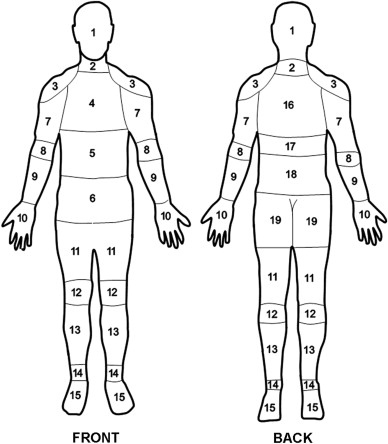
Select location of injury and answer the appropriate questions.
- 1 HEAD
- 2 NECK
- 3 SHOULDER
- 4 CHEST
- 5 STOMACH
- 6 ABDOMEN
- 7 UPPER ARM
- 8 ELBOW
- 9 LOWER ARM
- 10 HAND
- 11 HIPS, PELVIS, UPPER LEG
- 12 KNEE
- 13 LOWER LEG
- 14 ANKLE
- 15 FOOT
- 16 UPPER BACK
- 17 MID BACK
- 18 LOWER BACK
- 19 BUTTOCKS, TAILBONE
-
Describe nature of injury
-
Side
-
Provide pictures of the scene
-
Name of physician and hospital where treated
-
Name and phone number of Witness #1
-
Name and phone number of Witness #2
-
Foreman's Signature
-
Injured Employee's Signature