



Title Page
-
Site/Job
-
Date and Time of Audit
-
Prepared by
-
Location
1. EVENT DETAILS
-
Please click "Add Investigator" button.
Investigator
-
Investigator Name
-
Date and Time of the Event
-
Date First Reported
-
Date of this Report
EVENT TYPE AND DEFINITION
-
Hazard Report (no incident reported, complete report Follow-up)
-
Near Miss (any event/observation that could have resulted in injury or property damage)
-
Minor Harm Accident (Onsite First Aid treatment / potential future harm)
-
Harm Accident (Off site medical treatment and rehabilitation/ rest for not serious or permanent injury)
-
Serious Harm Injury (as defined by the act – refer to your policy before ticking)
-
Damage to Machinery / Property Plant / Equipment / Property Damaged Details
-
Has Work safe been notified?
-
What is a notifiable incident?
2. INVOLVED PERSONS
-
Please click "Add Name" button.
Name
-
Name of Injured / Near Miss Person
-
Employer
-
Please Specify
-
Name of Witness / Witnesses and Contact Phone Number(s)
-
Brief Summary of Event and Findings
-
Describe the Event
-
How was this allowed to happen within our company? (what processes were broken, safeguards non-existent, etc that allowed this to happen on our watch? List all that apply)
-
Training – Competency / Formal
-
Risk Assessments and Documentation
-
Equipment Involved
-
Process Failure
-
-
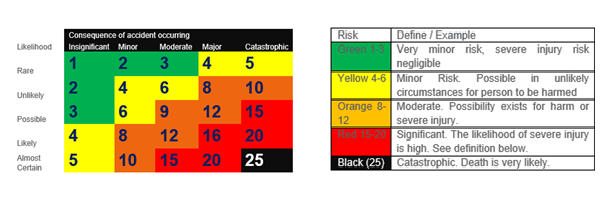
How Serious could this have been?
-
The likelihood of such an event reoccurring
-
If the event did reoccur, the likely consequence would be
-
The risk score is therefore
- Rare | Insignificant
- Rare | Minor
- Rare | Moderate
- Rare | Major
- Rare | Catastrophic
- Unlikely | Insignificant
- Unlikely | Minor
- Unlikely | Moderate
- Unlikely | Major
- Unlikely | Catastrophic
- Possible | Insignificant
- Possible | Minor
- Possible | Moderate
- Possible | Major
- Possible | Catastrophic
- Likely | Insignificant
- Likely | Minor
- Likely | Moderate
- Likely | Major
- Likely | Catastrophic
- Almost Certain | Insignificant
- Almost Certain | Minor
- Almost Certain | Moderate
- Almost Certain | Major
- Almost Certain | Catastrophic
3. TREATMENT AND FOLLOW-UP
-
What was the resulting injury?
-
What treatment was given to immediately address the issue?
-
Attach doctors/hospital report
-
What are the items used?
4. RESULTING ACTIONS
-
What can we do better to eliminate/minimize such an event reoccurring?
-
Tick items already actioned
-
Completed by Name and Signature
-
Date and Time of Completion
-
Include training and consider feedback from the investigation process in planning actions
-
Completed by Name and Signature
-
Date and Time of Completion
-
Refer to your policy to check if incident needs to be reported to Work Safe
-
Completed by Name and Signature
-
Date and Time of Completion
5. SUPPORTING MEDIA, DOCUMENTATION AND REPORTS
-
Please click "Add Item" button.
Item
-
Please Specify the item
-
Please put your comments here
-
Please upload a photo of the item
COMPLETION AND SIGN-OFF
-
Investigators Review and Sign-Off
-
Please click "Add Investigator" button.
Investigator
-
Investigator Name and Signature
-
Management Review and Sign Off
-
Manager Name and Signature