




Information
-
Plant
-
Department
-
Commenced on
-
Prepared by
Root Cause Analysis
Overview
-
This Template follows the process of the GF Problem Solving RCA Form. You may use some or all sections of the RCA form although the initial steps of identifying the issue must be completed.
The Process:
Complete an RCA with all findings recorded using this template.
Ensure follow up actions are allocated to someone.
Review actions for completion and effectiveness during the regular RCA review meeting.
The Review meeting decides when the RCA is fully completed and able to be signed off. -
Do you need further detail on how to complete an RCA ?
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
Description of the incident ( one phrase to identify this RCA and enable easy search in the future) Start with the equipment name followed by the issue eg. oven jam or Slicer blade break
-
Add a photo/s as required to help identify the issue and area.
-
Date and time
-
Shift
-
Name and Signature of person leading RCA
-
Name and Signature of person attending Note you can have multiple names and signatures if reqd in each box.
-
Name and Signature of person attending Note you can have multiple names and signatures if reqd in each box.
-
Name and Signature of person attending Note you can have multiple names and signatures if reqd in each box.
-
Name and Signature of person attending Note you can have multiple names and signatures if reqd in each box.
-
Name and Signature of person attending Note you can have multiple names and signatures if reqd in each box.
Step 1. Observe the problem firsthand, preferably as a Team. Get the facts. This is the most important step as all other steps depend on the accuracy of this step.
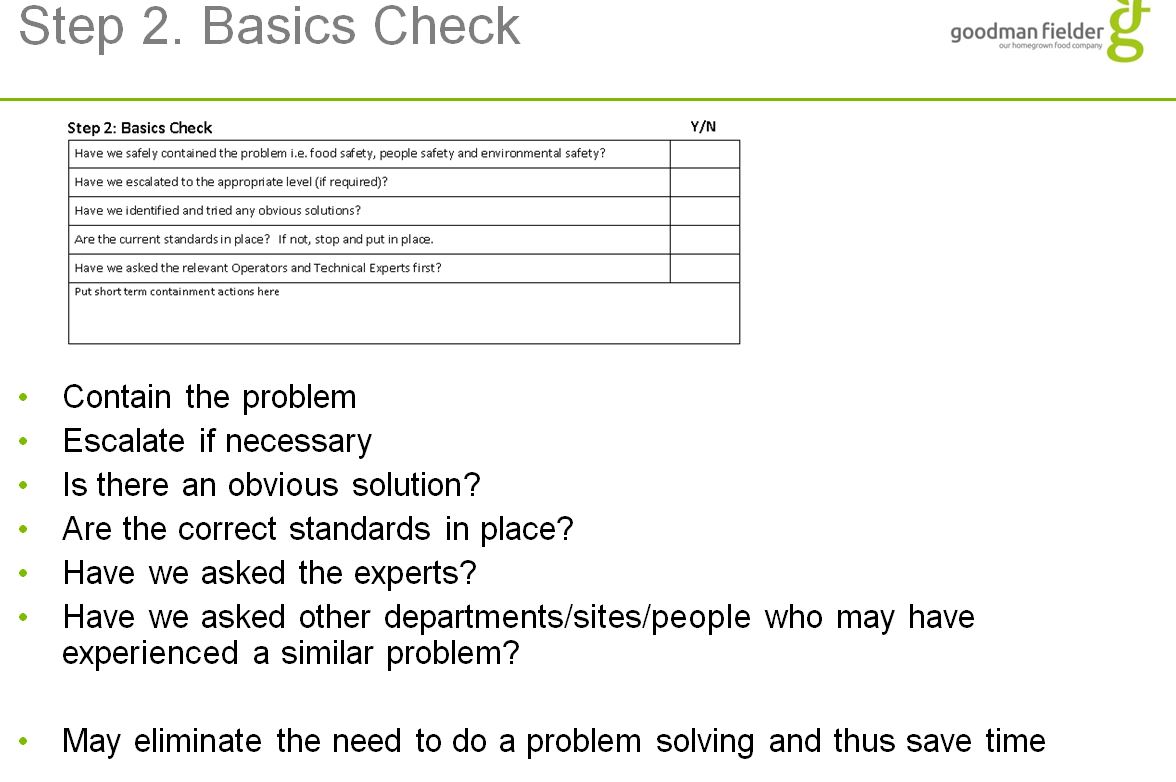
Step 2. Basics Check
-
Have we safely contained the problem i.e. food safety, people safety and environmental safety ?
-
Have we escalated to the appropriate level (if required)
-
Have we identified and tried any obvious solutions ?
-
Are the current standards in place ? If not, stop and put in place .
-
Have we asked the relevant Operators and Technical Experts first ?
-
Add any short term containment actions here.
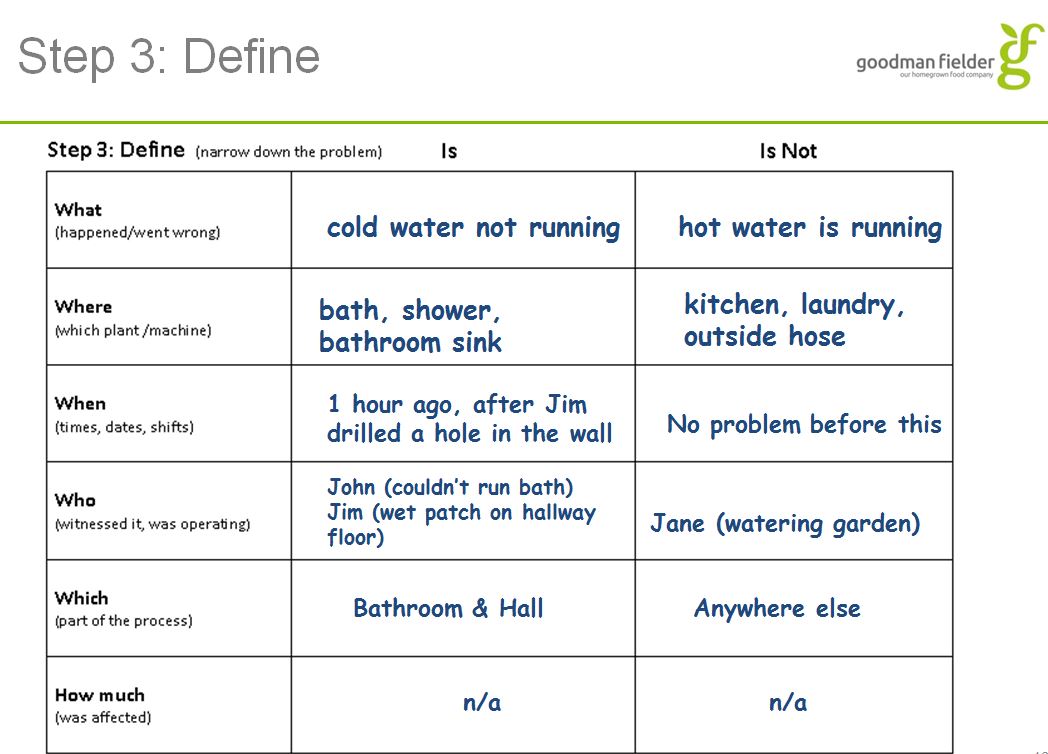
Step 3: Define (Narrow down the problem)
-
What (happened/went wrong) Define what it is and what it is not.....
-
Where (which plant/machine) Define what it is and what it is not.....
-
When (times/dates/shifts) Define what it is and what it is not.....
-
Who (witnesses/operators) Define who was involved and who was not.....
-
Which (part of the process or machinery) Define what it is and what it is not.....
-
How Much (was affected) Define what is and what it is not.....
-
Add photo/s as required to identify the problem.
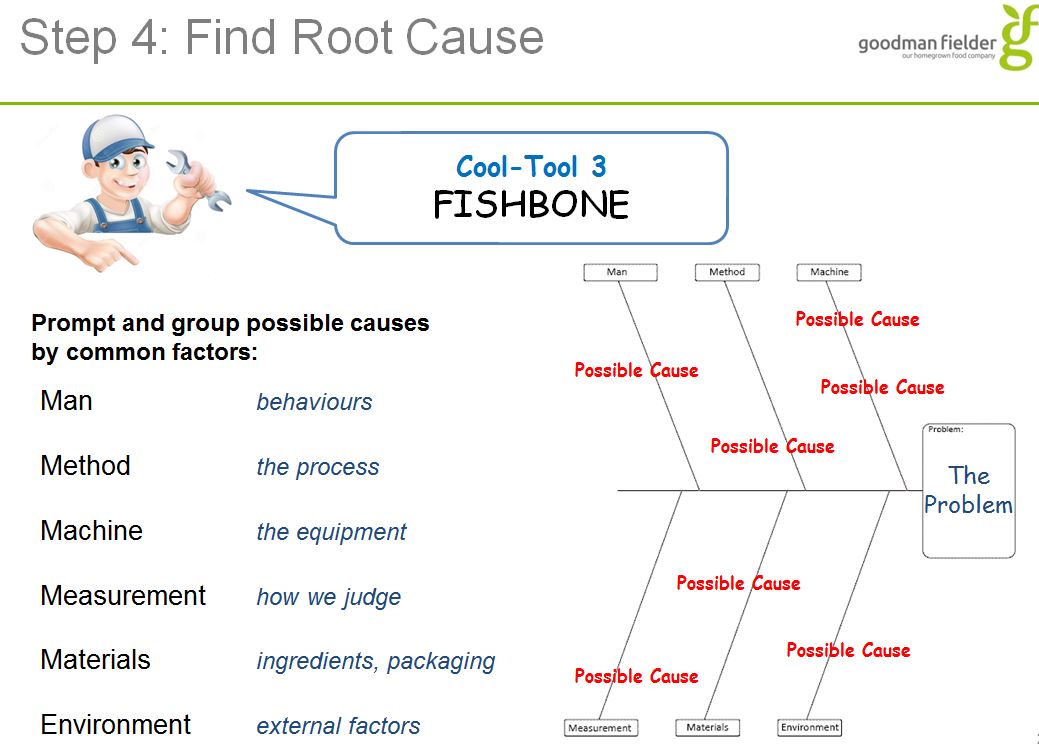
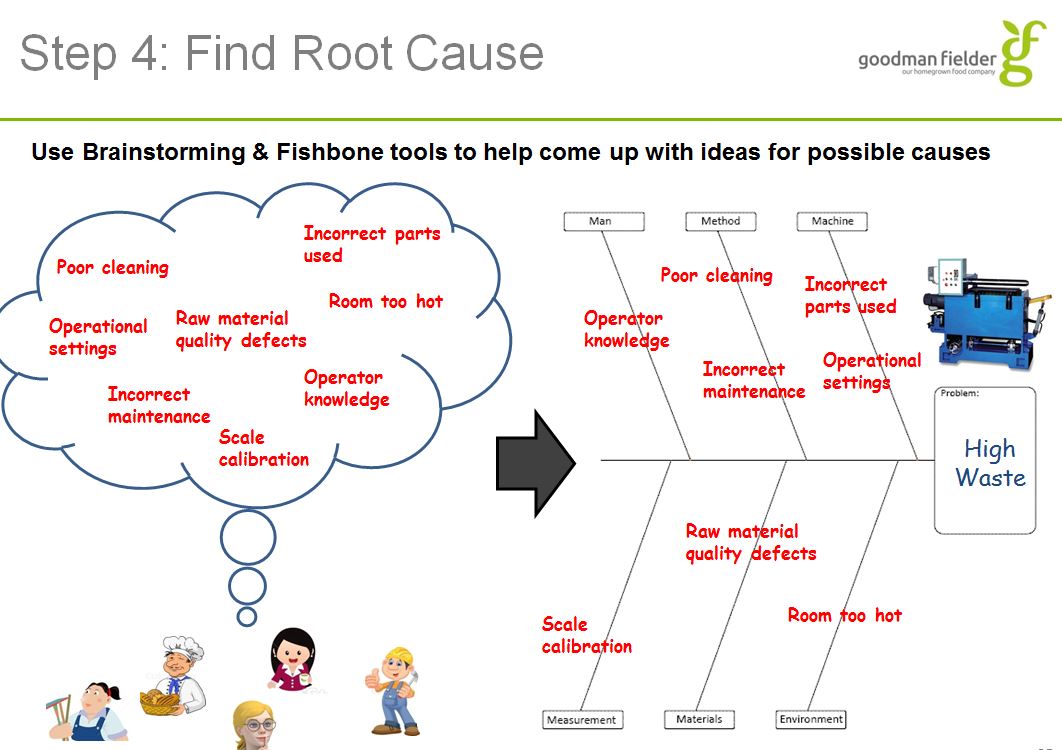
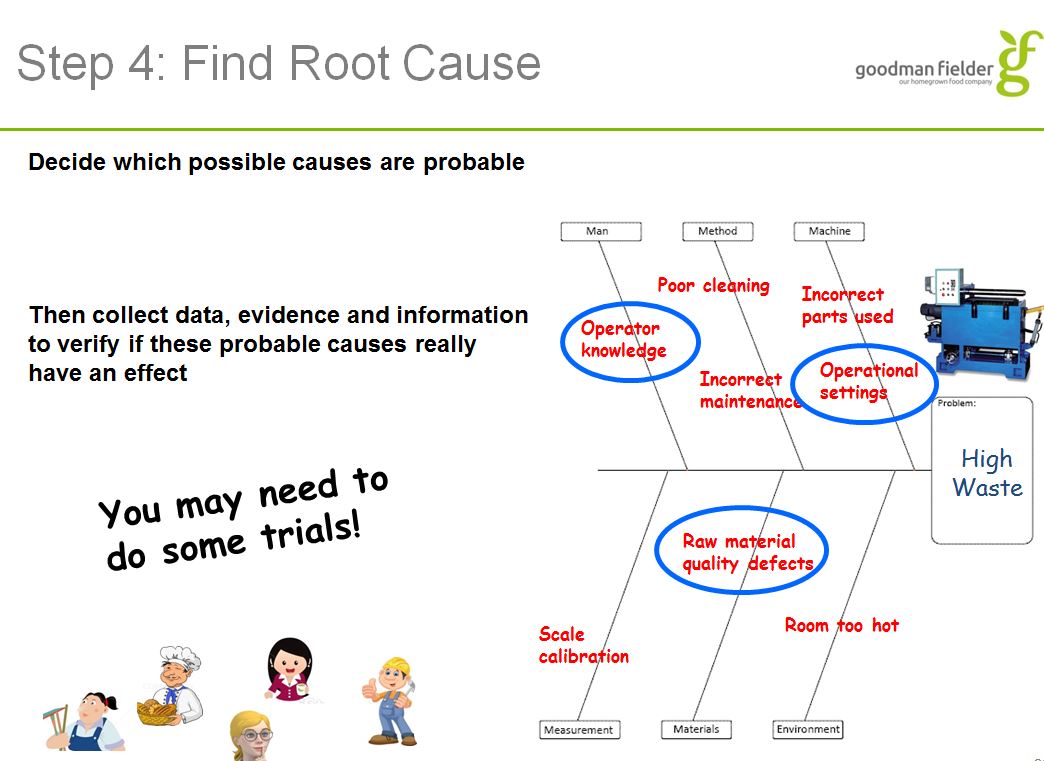
Step 4: Find Root Cause
-
For each Category here list possible causes as you would on a Fishbone (you may use a fishbone on a whiteboard or paper and then just add the single most probable or you can list every item. Add elements to provide data if reqd.
-
Add photos as required
Man
-
Add media
-
Add drawing
-
CONTRIBUTIVE FACTORS
-
BBS factors : * eyes not on task * mind not on task * fatigue * Overconfidence * line of fire * lack of balance
-
PPE : training provided efficient training verified
-
Communication : - supervisor to employee - employee to supervisor - employee to employee
-
MOST PROBABLE DIRECT CAUSE ( to be defined after completing the above elements, click add element as many times as needed then choose the most probable causes for this section. You can add photos, drawings or utilise the suggested contributing factors in each element. )
METHOD
-
Add media
-
Add drawing
-
CONTRIBUTIVE FACTORS
-
work permit
-
pre-op inspection
-
SOP
-
MOST PROBABLE DIRECT CAUSE ( to be defined after completing the above elements, click add element as many times as needed then choose the most probable causes for this section. You can add photos, drawings or utilise the suggested contributing factors in each element. )
MACHINE
-
Add media
-
Add drawing
-
CONTRIBUTIVE FACTORS
-
guarding inadequate machine guarding no guarding
-
Tools proper tool was not identified proper tool was not available
-
MOST PROBABLE DIRECT CAUSE ( to be defined after completing the above elements, click add element as many times as needed then choose the most probable causes for this section. You can add photos, drawings or utilise the suggested contributing factors in each element. )
MEASUREMENT
-
Add drawing
-
Add media
-
CONTRIBUTIVE FACTORS
-
calibration measurement
-
MOST PROBABLE DIRECT CAUSE ( to be defined after completing the above elements, click add element as many times as needed then choose the most probable causes for this section. You can add photos, drawings or utilise the suggested contributing factors in each element. )
MATERIAL
-
Add media
-
Add drawing
-
CONTRIBUTIVE FACTORS
-
recent process change
-
if chemical : SDS available
-
MOST PROBABLE DIRECT CAUSE ( to be defined after completing the above elements, click add element as many times as needed then choose the most probable causes for this section. You can add photos, drawings or utilise the suggested contributing factors in each element. )
ENVIRONMENT
-
Add drawing
-
Add media
-
CONTRIBUTIVE FACTORS
-
noise illumination floor walls
-
MOST PROBABLE DIRECT CAUSE ( to be defined after completing the above elements, click add element as many times as needed then choose the most probable causes for this section. You can add photos, drawings or utilise the suggested contributing factors in each element. )
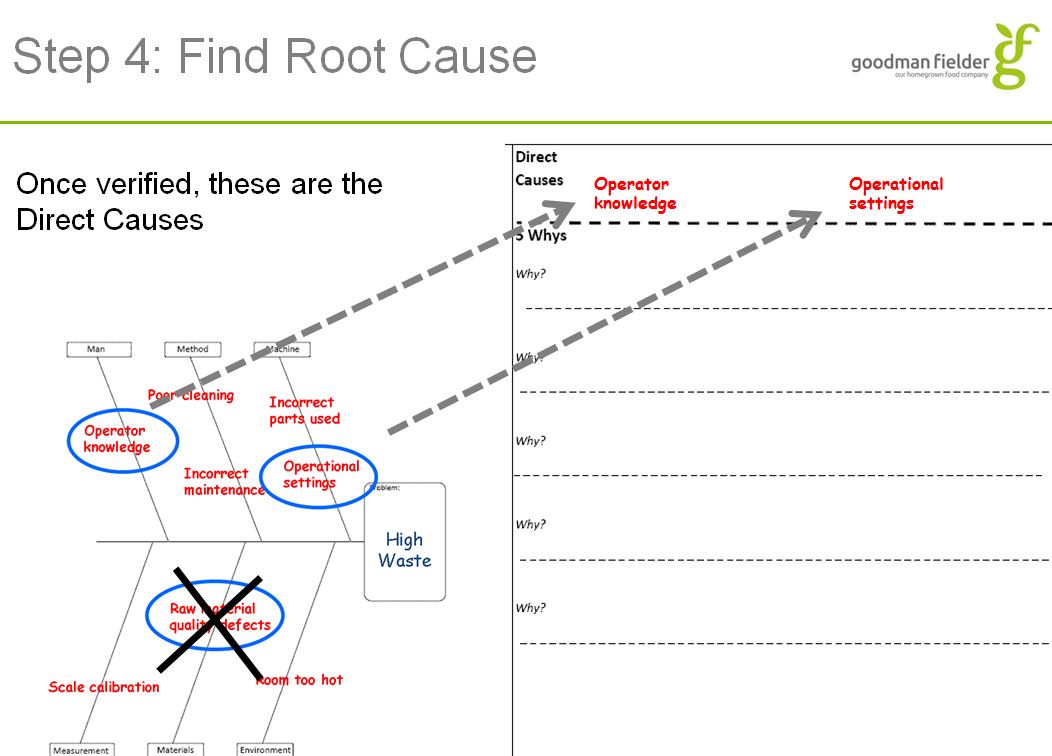
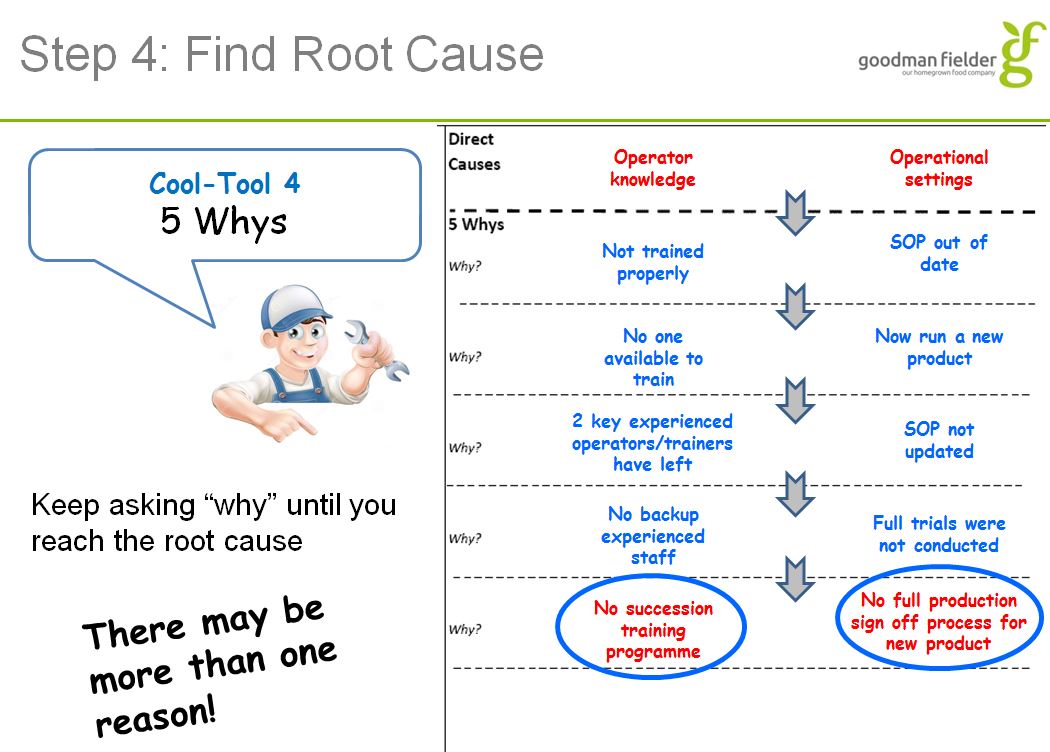
List Direct Causes most probable and conduct 5 Why Write most probable direct cause from above in first box. Ask Why ? up to 5 times to get to a Root Cause in the second box.
-
Why? Why? Why? Why? Why?
-
Probable Root Cause
List Direct Causes most probable and conduct 5 Why Write Root cause in first box. Ask Why ? up to 5 times to get to a Root Cause in the second box.
-
Why? Why? Why? Why? Why?
-
Probable Root Cause
List Direct Causes most probable and conduct 5 Why Write Root cause in first box. Ask Why ? up to 5 times to get to a Root Cause in the second box.
-
Why? Why? Why? Why? Why?
-
Probable Root Cause
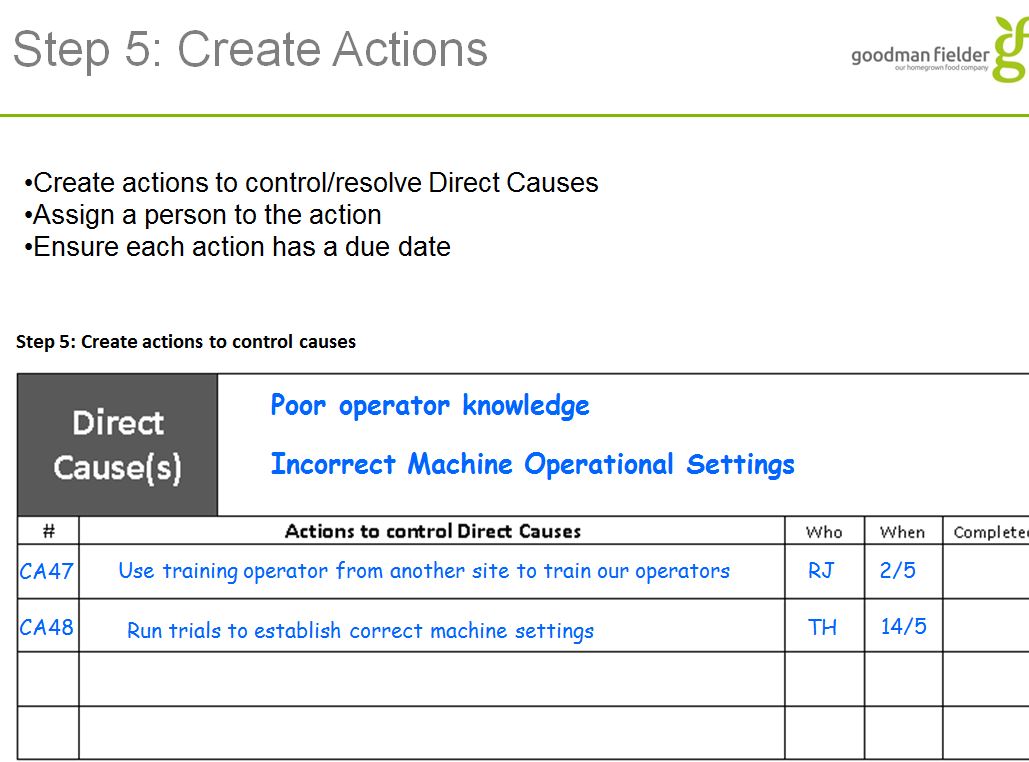
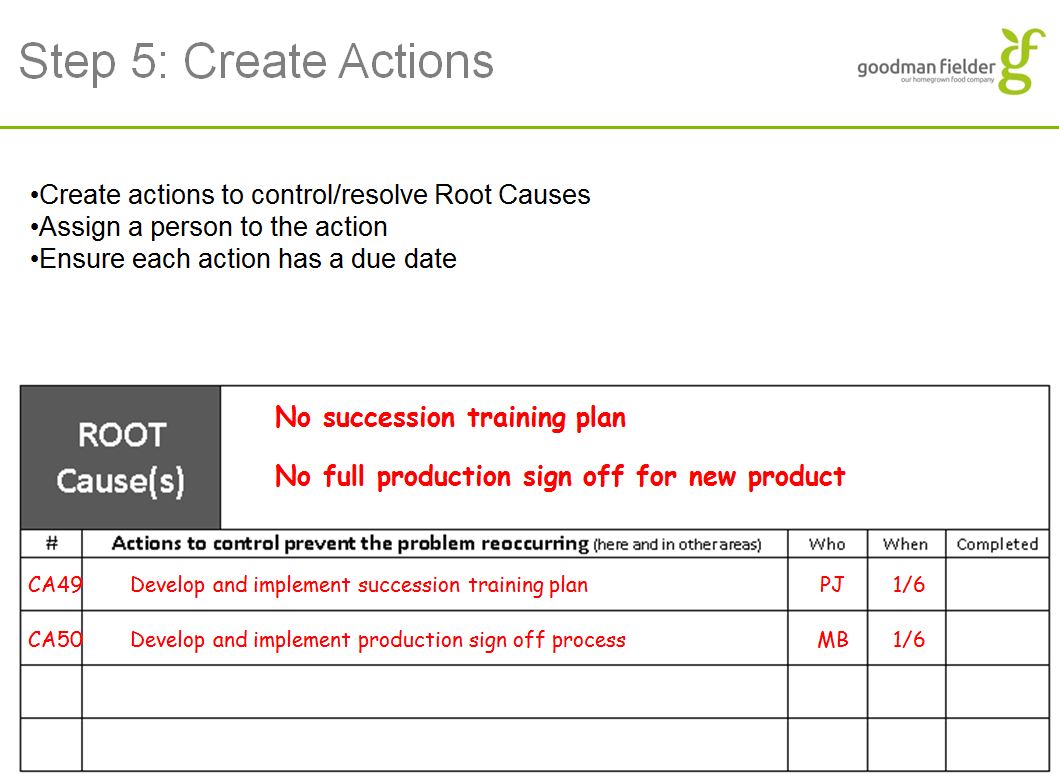
Step 5: Create Actions to control causes Corrective action Plan Add actions here as needed to address Direct Causes and Root Causes.
-
Action:
-
Responsible
-
Due Date
-
Follow up: completed ?
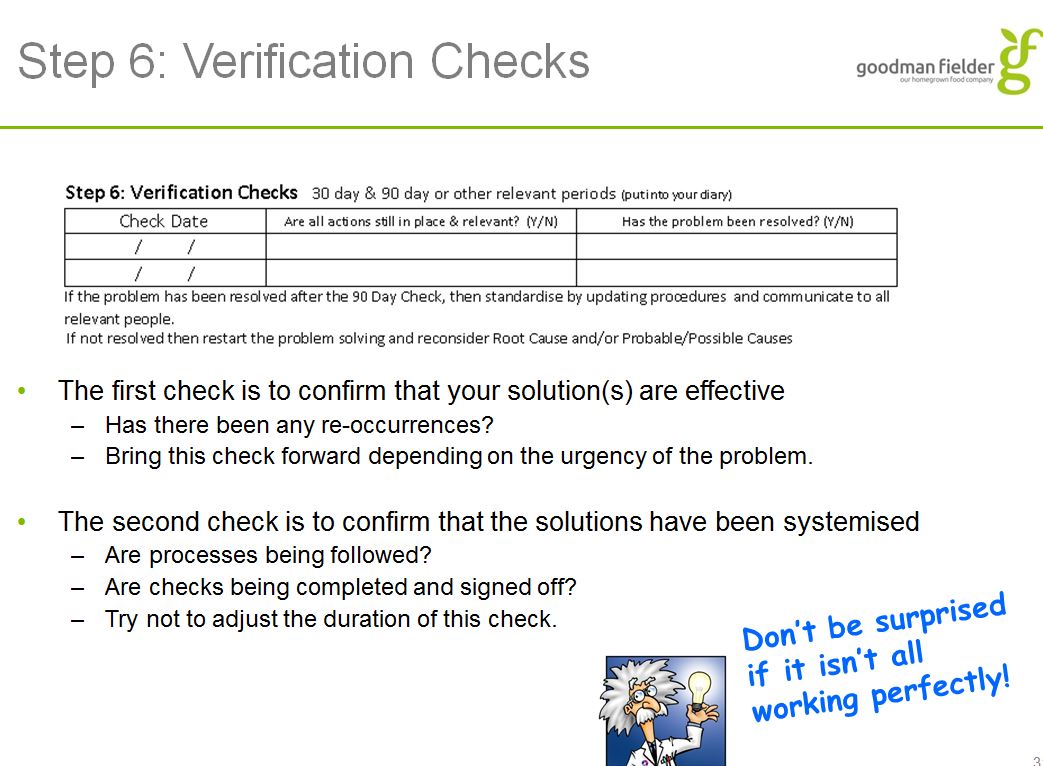
Step 6: Verification Checks
-
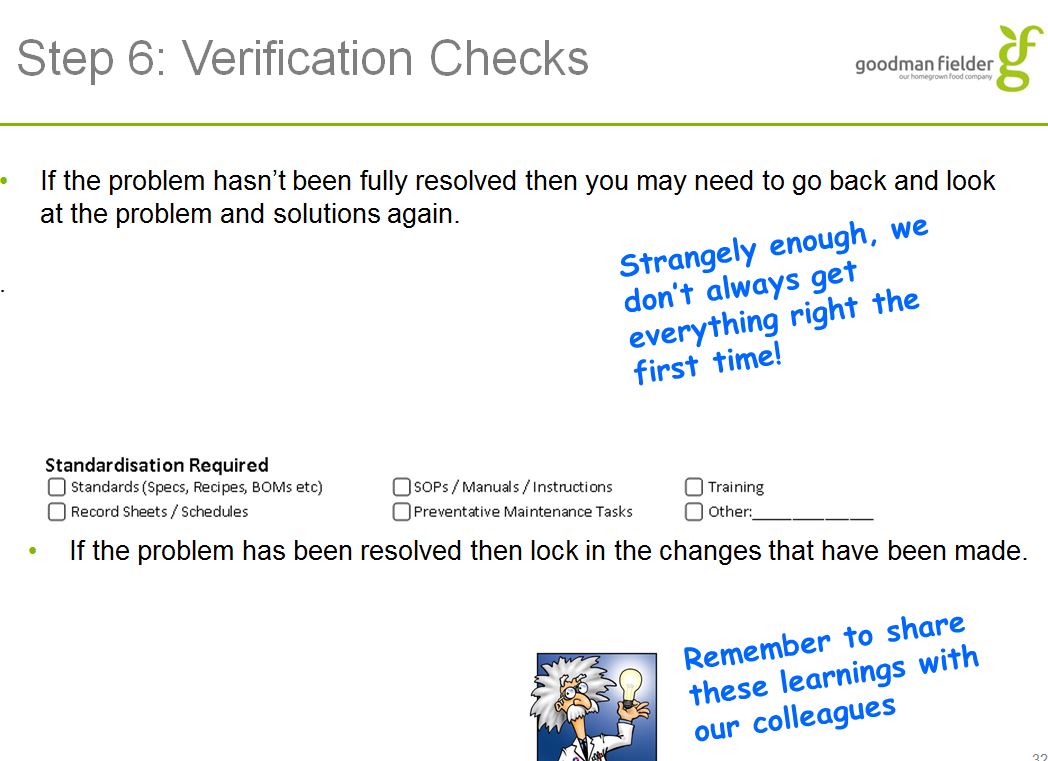
Is a 30 day and a 90 day check required ?<br>Using the "paperclip" on the right allocate an action to yourself or others in 30 days and 90 days for the following:<br>Are all actions still in place and relevant for (insert RCA detail) ?<br>Has the problem been resolved for (insert RCA detail) ?<br>For the 90 day check also annotate the following:<br>If problem is resolved standardise by updating procedures: Standards/SOPS/Training/Schedules/PMs or other
-
Do we need to incorporate 7Qs FMEA review if any proposed actions require PM changes ?<br><br>If yes an action box will appear to enable a specific action for this task.<br>
-
Action:
-
Responsible
-
Select date
-
Follow up: completed ?
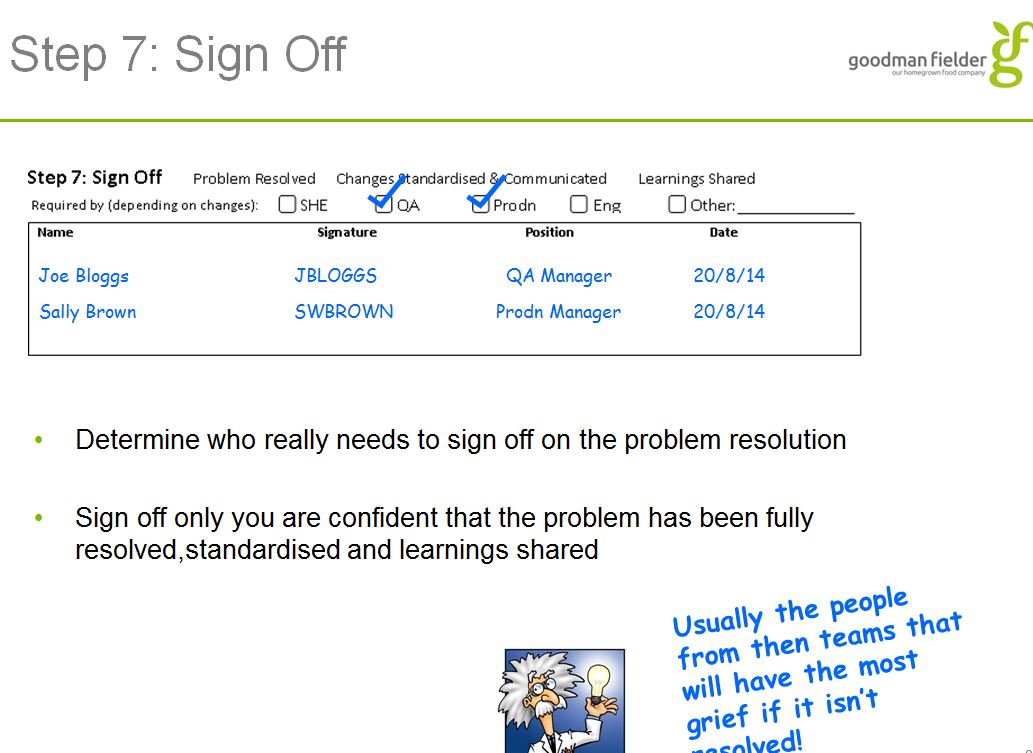
Step 7: Sign Off This is to remain open until Actions have been completed and it is decided in an RCA review meeting that the RCA is fully completed. The review meeting decides the appropriate signoff: Eg. SHS/QA/Production/Eng
-
Name and Signature of Signoff for RCA completion
-
Name and Signature of Signoff for RCA completion
-
Name and Signature of Signoff for RCA completion


")