




Information
-
Department
- 5 East
- 4 East
- 4 West
- Mental Health - Inpatient
- 4 North
- MDU
- PICU
- NICU
- Emergency
- Other
-
Please specify area audited:
-
Auditor Name
-
Conducted on
Hand Hygiene Observations
-
-
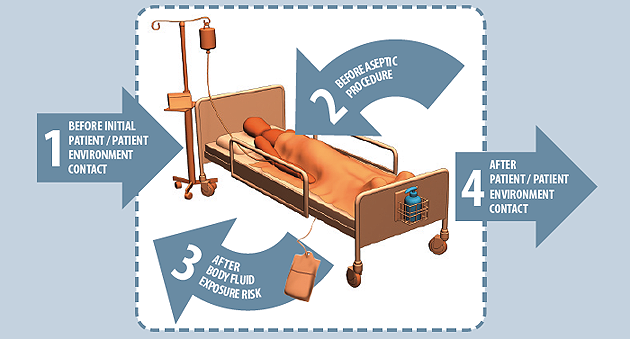
Which moment did you observe?
-
Was Hand Hygiene performed?
-
Describe:
Comments
-
Were there any barriers to Hand Hygiene identified or observed throughout this audit?





