Title Page
What report type you want to make ? (choose one)
-
Incident
-
Injury
-
Fleet / Asset
-
Hazard
Nature of report ? (choose one)
-
Near miss
-
Personal injury
-
Death
-
Asset damage
-
Assault
-
Physical threat
-
Verbal abuse
-
Other
-
Please describe the nature of report here
-
Date of incident / hazard
-
Name of person completing this form
-
Position
-
Phone number
-
email address
-
Location of the incident / hazard
-
Description of incident / hazard, how did it occur
-
Where there any contributing factors?
-
Is there any other witness for this incident / hazard report
-
Name of witness
-
Witness contact details
-
Any injured person ?
-
Name of the injured person
-
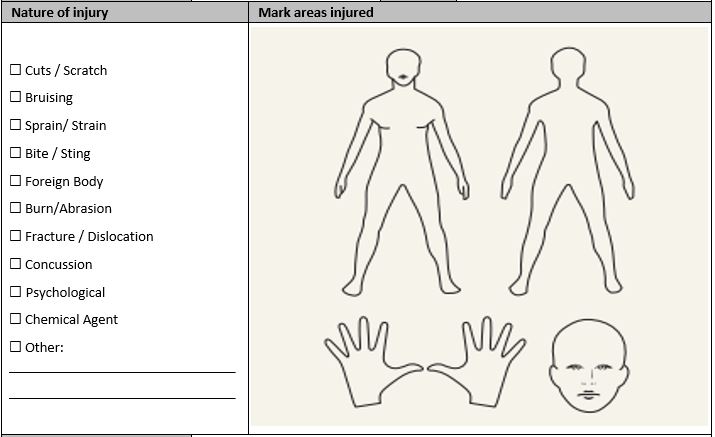
Describe the injury (which part of body, how bad is the injury etc.)
-
-
Injury treatment
-
No treatment
-
First aid treatment
-
Doctor / Medical centre
-
Hospital - outpatient
-
Hospital - Inpatient (kept overnight)
-
Other
-
Please describe the other treatment given here
-
Treatment details
-
Name of treatment provider
-
Treatment provider contact details
-
Do you have any recommendation for corrective action
-
List your suggestions here. What do you suggest happens so the incident / hazard does not occur again?
-
Signature of the person completing this form
-
Please send the completed incident report to your direct supervisor and whs@nlc.org.au within 24 hours of the incident occurring or hazard being identified.