




Information
-
Document No.
-
Audit Title
-
Client / Site
-
Conducted on
-
Prepared by
-
Location
-
Personnel
Personal Details
Your Personal Details
-
Full Name inc. Title:
-
Date of Birth:
-
How would you like to be addressed:
-
Address:
-
Home Telephone Number:
-
Mobile Telephone Number:
-
Preferred Language:
-
Do you require a Translator?
-
Religion / Beliefs:
Next of Kin Details
-
Name:
-
Relationship to you:
-
Address:
-
Home Telephone Number:
-
Work Telephone Number:
-
Mobile Telephone Number:
Emergency Contact Details - (if different from Next Of Kin)
-
Are they the same as 'Next of Kin'?
-
SEE NEXT OF KIN DETAILS
-
Name:
-
Relationship to you:
-
Primary Contact Number:
-
Secondary Contact Number:
GP Details
-
GP Name:
-
Surgery Name:
-
Surgery Address:
-
Telephone Number:
-
Out of Hours Telephone Number:
Care Manager / Social Worker Details
-
Name:
-
Address:
-
Office Telephone:
-
Out of Hours Telephone:
Funding Details
-
Date Paperwork Received:
-
Social Services Review Date:
-
Funding Sources:
-
Total Care / Support Hours Required:
Existing Support
What Existing Care / Support do you Currently Receive? Details of any Existing Care / Support you currently receive: (name of person/organisation - contact details inc address - type of Care/ Support and days/times)
-
Details:
About You and Your Life History
About You and Your Life History - Note: Consider things such as Birth Place, Growing Up, Work, Family, Relationships, Significant Dates, Interests/Hobbies, TV Programs, Books/Papers, Food & Drink likes/Dislikes):
-
Details:
Medical and Medication
Medical and Medication Information
-
Known Allergies
-
Medical History
-
Does the Service User take Medication?
-
Current Types of Medication (Consideration MUST be given to the type of Medication and level of Staff Interaction as some Medication Types and Administration Methods will require 'Specialist Training')
- Liquid;
- Tablet;
- Inhaler;
- Patch;
- Injected;
- Eye Drops;
- Ear Drops;
- Cream;
- Other;
-
List ALL Current Medications: (see MAR Sheet for details etc.)
-
Medication Dispensing:
- MDS
- Bottle
- Measure
- Doset Box
-
Does the Service User Self Medicate?
-
Complete a 'Medication Self Assessment' form
-
Are Staff Required To have involvement with Service User Medication?
-
What Level of Input will be required by Staff?
- PROMPT
- ASSIST
- ADMINISTER
-
Does any Medication Assistance require Staff to have 'Specialist Training'?
-
Specialist Training Requirements:
-
Are there any 'Special' Training Requirements as per Local Authority?
-
Local Authority Requirements:
-
Is a MAR Chart in Place and Ready for use?
-
CONTACT OFFICE TO ARRANGE FOR MAR CHART BEFORE COMPLETING THIS SECTION
-
Difficulties taking Medication e.g. Swallowing, Spilling Liquid Meds etc?
-
Details of any Difficulties:
-
Does Management of Prescribed or Un-Prescribed Medication(s) have 'Potential' to Cause Risk?
-
Details of any Potential Risks:
-
Is All Appropriate Documentation On File? e.g. MAR Sheets, Controlled Drugs Records, Disposal Forms etc.
-
Details of requirements:
-
Are there any 'Controlled Drugs' on the premises?
-
Are they Adequately Stored?
-
Details of Storage Improvement Requirements:
-
Is a 'Consent to Treatment' Form required? (Mental Health)
-
COMPLETE A 'CONSENT TO TREATMENT' FORM BEFORE COMPLETING THIS SECTION
-
Any Relevant Notes or Information:
Skin Care
Skin Care and Pressure Care
-
Are there any Skin Care Concerns at this time?
-
Describe Skin Care Concern:
-
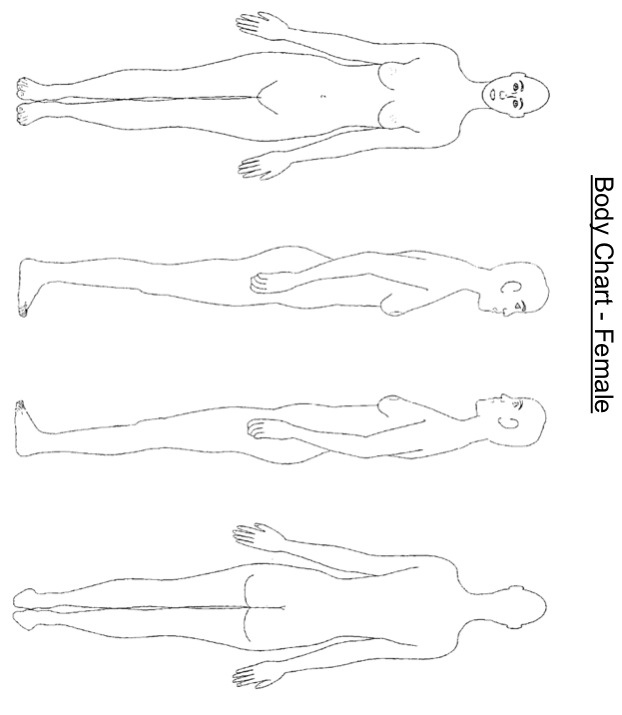
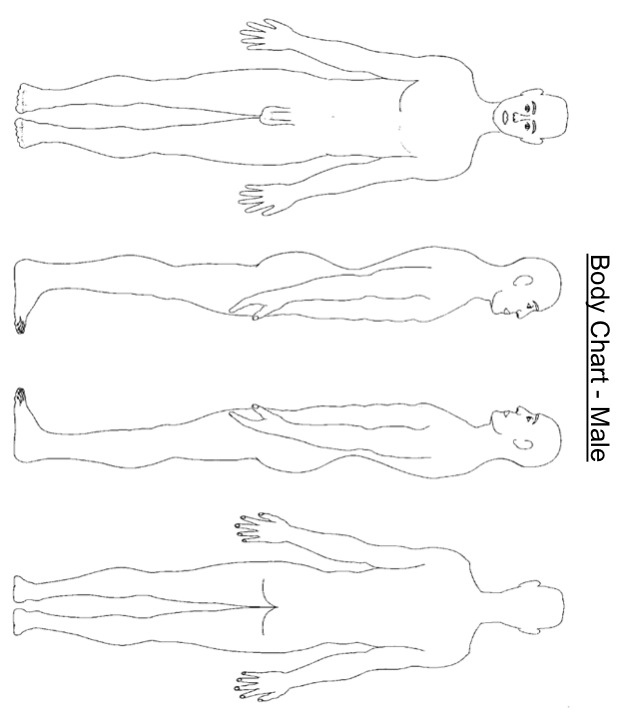
CLEARLY IDENTIFY ON BODY CHART (Photograph if possible)
-
Select Chart
-
Complete chart when Printed
-
Complete Chart when Printed
-
Media
-
Skin Care Products to use:
-
Describe Skin Care Routine:
-
Any Relevant Notes or Information:
-
Are there any Pressure Care issues at this time?
-
Describe Pressure Care concern:
-
CLEARLY IDENTIFY ON BODY CHART (Photograph if possible)
-
Select Chart
-
Complete chart when Printed
-
Complete Chart when Printed
-
Media
-
What pressure Care Aids are to be used?
-
Describe Pressure Care Routine:
-
Is a 'Turns Monitoring' Form Required?
-
Has the Turns Monitoring form been Completed and included with the Care Plan?
-
Any Relevant Notes or Information:
Sight - Hearing - Communication
Sight - Hearing - Communication
Sight
-
Service Users Sight is:
-
Does the Service User Wear Glasses?
-
Glasses required:
-
Other Relevant Information: (contact lenses etc)
-
Any Relevant Notes or Information:
Hearing
-
Service Users Hearing is:
-
Is a Hearing Aid or Hearing Device Used?
-
Details of Devices Used:
-
Any Relevant Notes or Information:
Communication
-
Service Users Levels of Verbal Communication and Conversation are:
- Full
- Partial
- None
-
Do they Respond Well to YES / NO Type Questions?
-
What other types of Communication can be used? (Picture/Note Pad/Sign etc)
-
Any Relevant Notes or Information:
Mobility and Dexterity
Mobility and Dexterity
-
Able to Walk Unaided?
-
Requires the use of the following items:
- Wheelchair
- Frame
- Stick
- Calliper
- Brace
-
Is there a Risk relating to any of the Mobility Aids?
-
MOBILITY AID RISK ASSESSMENT and MANAGEMENT PLAN COMPLETED?
-
Able to answer the Door to Allow Care Staff In?
-
Details of how Care Staff will Gain Entry to the Premises: (e.g. Key Safe, Key Holding, someone present etc)
-
Able to Go Out Alone?
-
Will Staff be required to assist the Service User on External Activities?
-
Complete an 'EXTERNAL RISK ASSESSMENT' Form
-
Any Relevant Notes or Information:
Falls
-
Has the Service User 'Fallen' in the Past 12 months?
-
Record Details and complete a 'Falls Risk Assessment' Form
-
Any Relevant Notes or Information:
Showering/Bathing/Grooming
Personal Hygiene Routines
Showering / Bathing
-
Service User Prefers:
- Shower
- Bath
- Bed Sponge
- Flannel Wash
-
Service User is:
-
Bathing Risk Assessment Completed?
-
Details of Preferred Frequency & Day / Time:
-
Showering / Bathing Aids:
- Hoist
- Shower Chair
- Bath Seat
- Other
-
Details of Other:
-
Details of Preferred Toileteries:
-
Any Relevant Notes or Information:
Hair Care
-
Service User is:
- Independent
- Prompted
- Supervised
- Some Assistance
- Fully Assisted
-
Hair Dresser Frequency and Details:
-
Facial Hair
-
Service User Prefers:
- Wet Shave
- Electric Shave
- Other
-
Details of Other:
-
Shaving Frequency and Details:
-
Details of any Other Hair Removal Requirements:
-
Any Relevant Notes or Information:
Oral Hygiene Routine
-
Own Teeth:
-
Details of Teeth:
-
Dentures:
- None
- Partial
- Full Upper
- Full Lower
-
Details of Dentures:
-
At Night, Dentures are to be:
- In
- Out
-
Any Relevant Notes or Information:
Foot Care
-
Service User is:
- Independent
- Prompted
- Supervised
- Some Assistance
- Fully Assisted
-
Details of Foot Care Routines & any Specialist Treatment:
-
Any Relevant Notes or Information:
Dressing / Undressing
Dressing and Undressing Requirements
-
Service User is:
-
Details of All Assistance Required:
-
Any Relevant Notes or Information:
Continence Needs
Continence Requirements
-
Toileting Regime:
- Independent
- Prompted
- Supervised
- Some Assistance
- Fully Assisted
Bladder Management
-
Service User is:
-
Management Aids:
- Pads
- Pants
- Kylie Sheets
- Catheter
- Other
-
Details of Incontinence:
-
Catheter Management Plan:
-
Toileting Aids:
- None
- Over Toilet Frame
- Raised Seat
- Commode
- Bed Pan
- Uridome
-
Details of Specific Toilet Times / Routines:
-
Any Relevant Notes or Information:
Bowel Management
-
Service User is:
-
Management Aids:
- Pads
- Pants
- Kylie Sheets
- Catheter
- Other
-
Details of Incontinence:
-
Details of Specific Toilet Times / Routines:
-
Any Relevant Notes or Information:
Eating and Drinking
Eating and Drinking Requirements
-
Are there any Enteral (PEG/NGT) Feeding Requirements?
-
Give detailed information as to requirements:
-
Prefers to have Meals in their:
- Kitchen
- Dining Room
- Lounge
- Bedroom
- Other
-
Details:
-
For Eating, the Service User is:
-
Service User is:
- Right Handed
- Left Handed
-
Type of Diet is:
- Normal
- Soft
- Modified Soft (minced)
- Puréed
- Other
-
Details:
-
Is there a requirement for a 'Special Diet'? (Low Fat, High Fibre etc)
-
Details of 'Special Diet'
-
Are there any foods the Service User SHOULD NOT Consume?
-
Give full details of food items the Service User may not consume and reasons why:
-
Is there a requirement for and specific Eating Aids?
-
Give Full Details:
-
For Drinking, the Service User is:
-
Do they have a 'Preferred' drink?
-
Details of Drinks:
-
Is there a requirement to use a 'Thickener' ?
-
Details of Thickener required:
-
Are any 'Drinking Aids' required?
-
Give Details of Drinking Aids:
-
Any Relevant Notes or Information:
Domestic Needs
Domestic Needs - Meals and Meal Preperation
-
For Preparing / Cooking / Heating Meals, the Service User is:
-
Are there any known Food Allergies:
-
Give details of foods to avoid:
-
Details of Preferred Meals and Times:
-
For preparing Drinks, the Service User is:
-
Details of Preferred Drinks and Times:
Domestic Needs - Housework
-
Will Staff be required to undertake General Cleaning duties?
-
Details all Cleaning duties:
-
COSHH Risk Assessment Completed?
-
Any Relevant Notes or Information:
Domestic Needs - Beds
-
Will Staff be required to make / change beds?
-
Details of Routine and Requirements:
-
Any Relevant Notes or Information:
Domestic Needs - Laundry
-
Will Staff be required to undertake Laundry duties?
-
Details of Routine / Detergents / Drying etc.
-
COSHH Risk Assessment Completed?
-
Any Relevant Notes or Information:
Domestic Needs - Shopping
-
Will Staff be required to undertake Shopping duties?
-
Is a 'Financial Record' form in place?
-
Details of Shopping Requirements inc. Days / Times / Locations etc:
-
Any Relevant Notes or Information:
Sleeping and Settling
Sleeping and Settling Requirements
-
Usual Time to Rise:
-
Usual Time to Bed:
-
Daytime Rest Routine:
-
Preferred Sleeping Position:
- No Preference
- Back
- Front
- Left Side
- Right Side
-
Preferences for Bed Coverings / Pillows etc.
-
Sleeping Aids:
- None
- Massage
- Music
- Radio
- Hot Pack
- Other
- Warm Drink
- Cold Drink
- Snack
-
Sleeping Aids Details:
-
Room Preferences:
- Light On
- Light Off
- Night Light
- Door Open
- Door Closed
- Window Open
- Window Closed
- Bed Rails Up
-
Complete a Bed Rail Risk Assessment
-
Night Time Patterns:(e.g. Wanders/Talks/Shouts etc.)
-
Details of any Night Time Checks Required:
-
Any Relevant Notes or Information:
Finances
Finances and Advanced Decisions
-
Does the Service User manage their own finances
-
Contact details for Finance Management:
-
Have they made any Advanced Decisions?
-
Contact details of responsible Person:
-
Have they prepared a Will?
-
Contact details of responsible Person:
Emotional Wellbeing
Emotional and Mental Wellbeing
-
Do you have any Emotional Wellbeing or Mental Health considerations?
- Emotional
- Mental
- No Concerns
-
Do identified Emotional Wellbeing considerations have potential to cause a risk?
-
Has a 'Triggers and Precipitating Factors' form been completed
-
Who is at Risk?
- Self
- Staff
- Visitors
-
Give Full Details:
-
What is the Level of Risk?
-
Complete a 'Risk Management Plan'
-
Do identified Mental Health considerations have potential to cause a risk?
-
Has a 'Triggers and Precipitating Factors' form been completed
-
Who is at Risk?
- Self
- Staff
- Visitors
-
Give Full Details:
-
What is the Level of Risk?
-
Complete a 'Risk Management Plan'
-
Is there a risk of 'Wandering'?
-
Details:
-
Is a Full Risk Assessment and Management Plan completed?
Risk Assessments
Risk Assessments
General and Physical Health
-
Do you have any General or Physical Health Considerations?
-
Details:
-
Do the above considerations have the potential to cause Risk?
-
Details:
-
Is there a Risk of Injury from Slips or Falls?
-
Details:
Falls Risk Assessment
-
Age:
-
Mobility:
-
History of Falls?
-
Sensory Impairment:
-
Other Factors
-
Medication Side Effects?
-
Loss of Sensation?
-
Oedema Lower Limbs?
-
Short of Breath?
-
Dizzy or Light-Headedness?
-
Pain?
-
Muscle Wastage or Weakness?
-
Incontinence and tries to rush to toilet?
-
Problems with Balance?
-
Confusion or Aggression?
-
Poor Fitting Footwear?
-
Wanderer?
-
Trip Hazards around home?
-
Select Total Score:
- -1
- 0
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
-
Is the Score Lower than 14?
-
Service User is Low Risk and No Management Plan is required at this time.
-
Is the Score Lower than 8?
-
Service Users with a score of 8 or BELOW ARE AT HIGH RISK..!!!
Review Care Plan provision and consider the person to be a High Dependency Service User
Review Staffing input requirement.. -
Complete a Falls Risk Management Plan for a HIGH RISK Service User.
-
Complete a Falls Risk Management plan for a MEDIUM RISK Service User
-
Service Users with a score of 13 or BELOW ARE AT RISK..!!!
Condition and Care Plan should be monitored closely and staff should ensure that the Service User has all necessary personal items close to hand to minimise risks. -
Select date
-
Staff Member Completing:
-
Is there a Risk Relating to the use of Mobility Aids?
-
Complete a MOBILITY AID RISK ASSESSMENT
-
Is there a requirement for a Moving & Handling Risk Assessment?
-
Complete a MOVING & HANDLING RISK ASSESSMENT
-
Is there a requirement to Assist with Bathing & Showering?
-
Complete a BATHING & SHOWERING RISK ASSESSMENT
-
Is there a Risk from Smoking?
-
Complete a SMOKING RISK ASSESSMENT
-
Is there a requirement for an 'External Activities' Risk Assessment?
-
Complete an EXTERNAL ACTIVITIES RISK ASSESSMENT
-
Any relevant Notes or Information