




Title Page
-
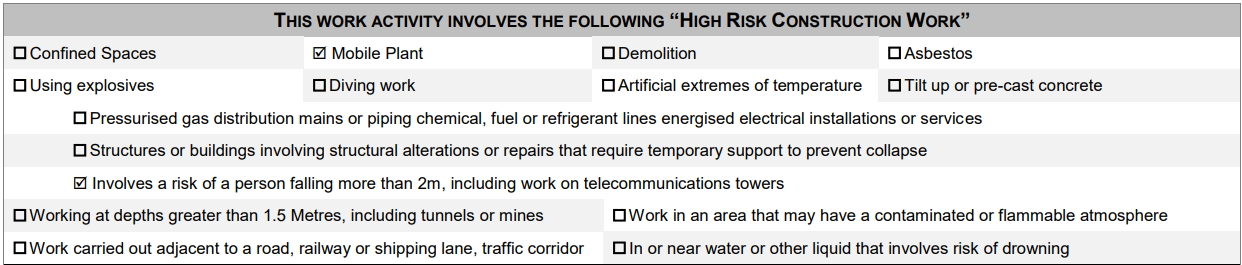
ACTIVITY: Roof Edge Protection
-
SWMS #
-
BUSINESS NAME:
-
BUSINESS ADDRESS:
-
ABN:
-
BUSINESS CONTACT:
-
PHONE #:
SWMS PART 1
SWMS APPROVED BY: EMPLOYER / PCBU / DIRECTOR / OWNER
-
NAME AND SIGNATURE:
-
DATE:
-
PERSON/S RESPONSIBLE FOR ENSURING COMPLIANCE WITH SWMS: TIFFANY GILCHRIST, ROSS GREY, ADRIAN BLACK
PERSON/S RESPONSIBLE FOR REVIEWING THE SWMS:
-
RELEVANT WORKERS CONSULTED IN THE DEVELOPMENT, APPROVAL AND COMMUNICATION OF THIS SWMS.
-
NAME AND SIGNATURE:
-
DATE:
ALL PERSONS INVOLVED IN THE TASK MUST HAVE THIS SWMS COMMUNICATED TO THEM BEFORE WORK COMMENCES.
-
Daily Tool Box Talks will be undertaken to identify, control and communicate additional site hazards. Work must cease immediately if incident or near miss occurs. SWMS must be amended in consultation with relevant persons. Amendments must be approved by ____Adrian Black, Ross Grey__________ and communicated to all affected workers before work resumes. SWMS must be made available for inspection or review as required by WHS legislation. Record of SWMS must be kept as required by WHS legislation (until job is complete or for 2 years if involved in a notifiable incident).
PRINCIPAL CONTRACTOR DETAILS (The builder or the organisation you are working for.)
-
PRINCIPAL CONTRACTOR (PC):
-
PROJECT NAME:
-
DATE SWMS PROVIDED TO PC:
-
PROJECT MANAGER (PM)
-
CONTACT PH. #:
-
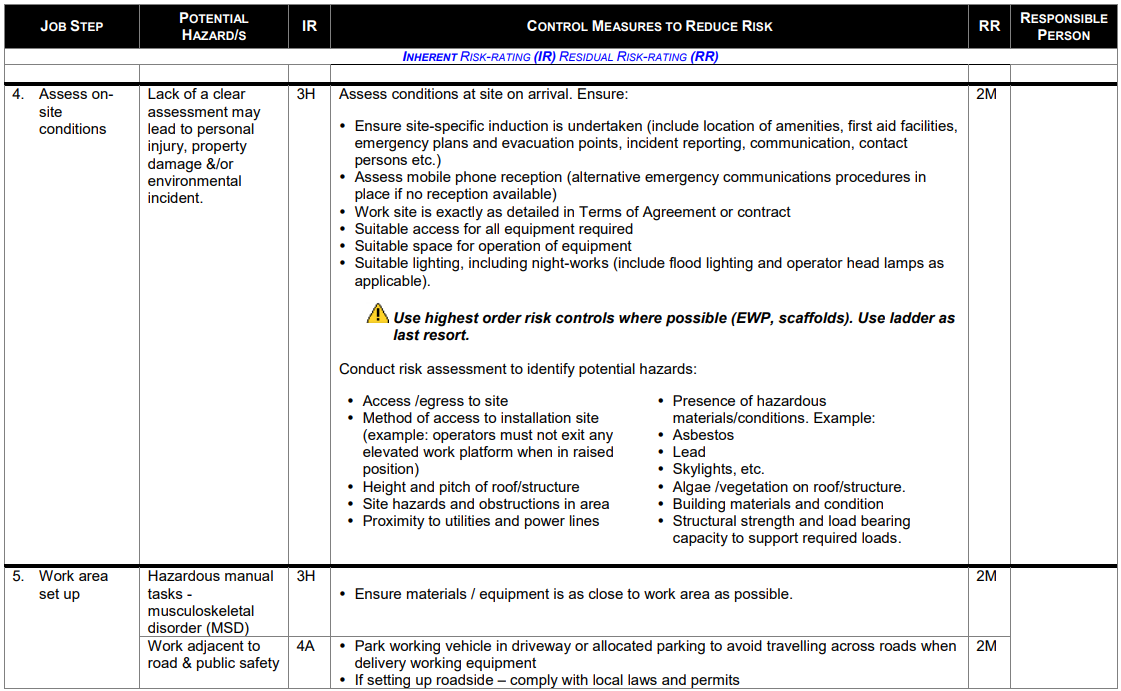
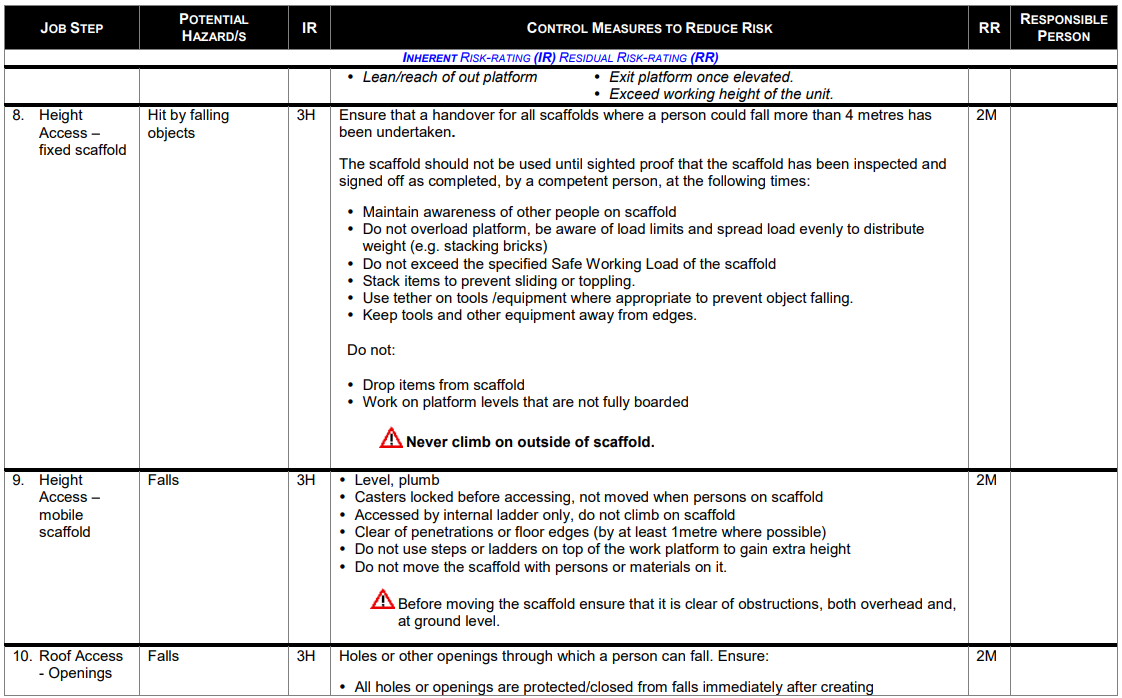
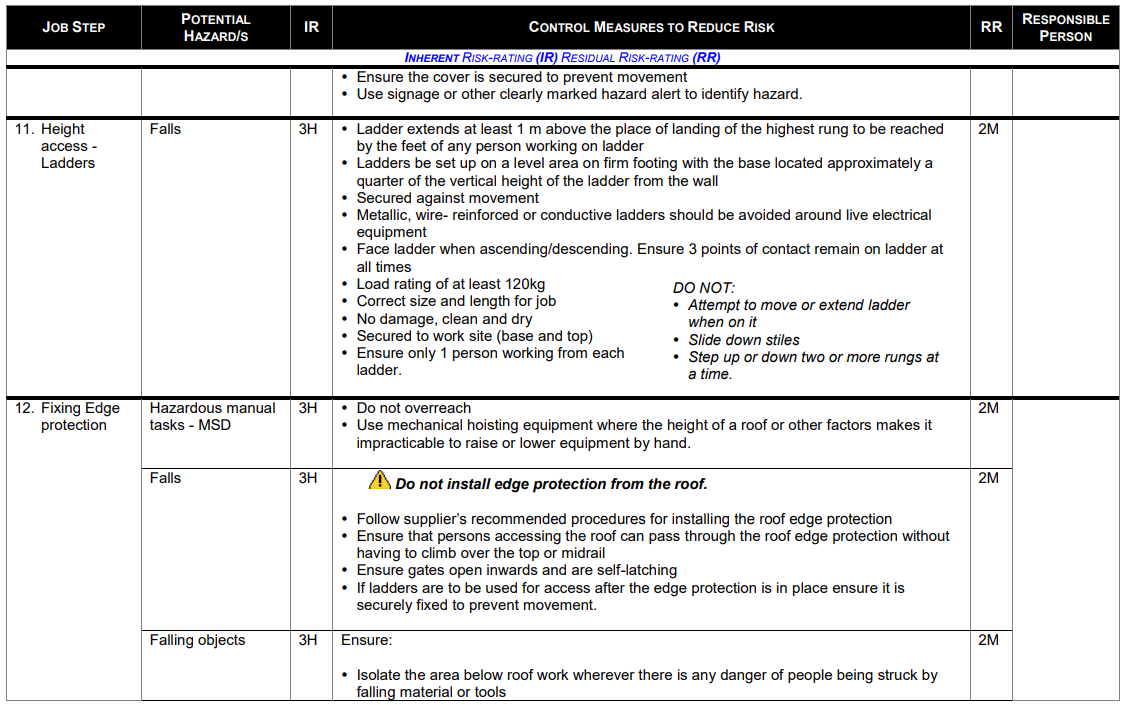
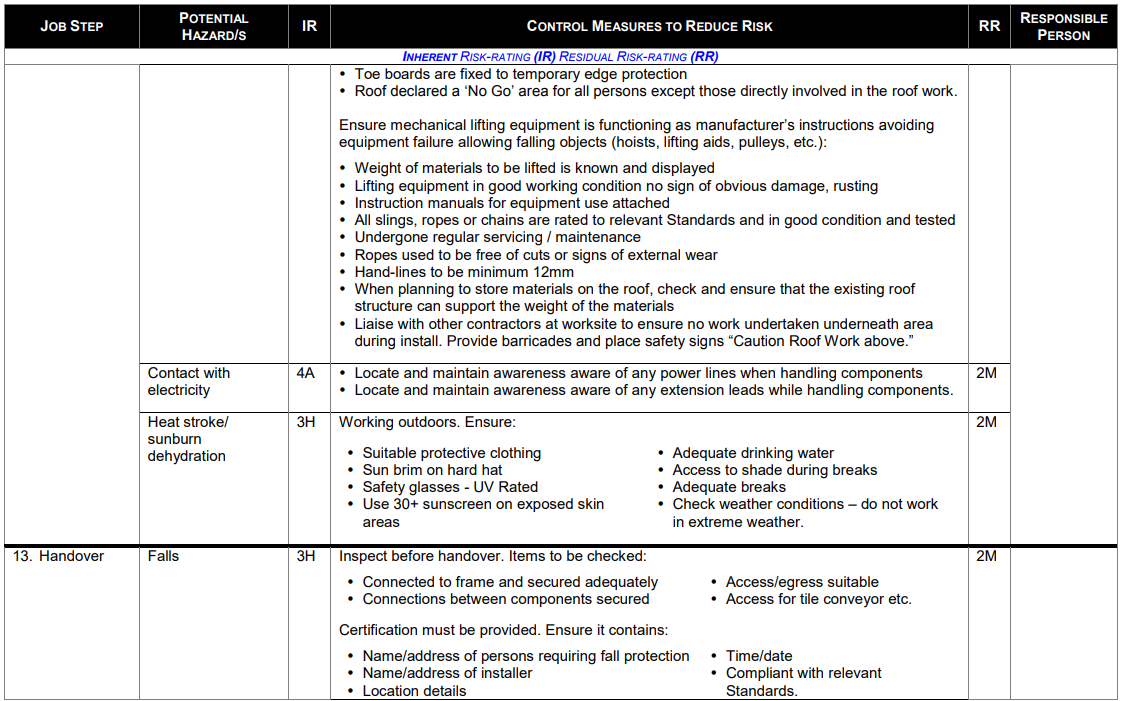
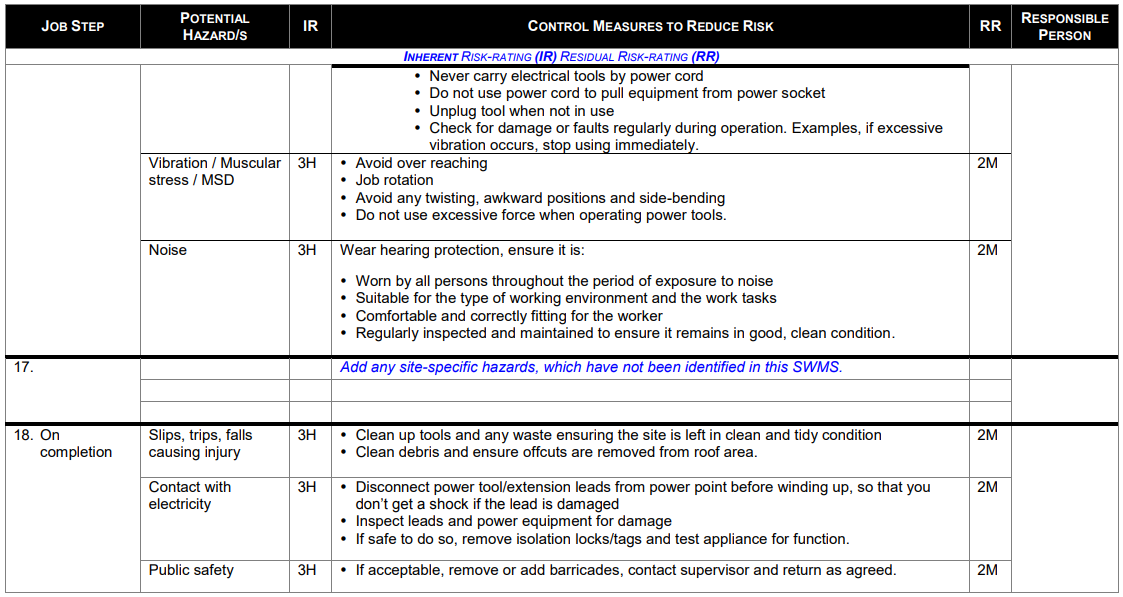
SWMS SCOPE: This SWMS covers general aspects associated with installation, use and subsequent dismantling of roof edge protection systems.
This SWMS does not cover the specific setup of height access equipment. A dedicated SWMS will be required for the set-up/erection of height access equipment such as Mobile and Fixed Scaffolds, Mobile Elevated Work Platforms etc. -
-
PERSONAL PROTECTIVE EQUIPMENT (PPE):
-
ENSURE ALL PPE MEETS RELEVANT AUSTRALIAN STANDARDS. INSPECT, AND REPLACE PPE AS NEEDED.
-

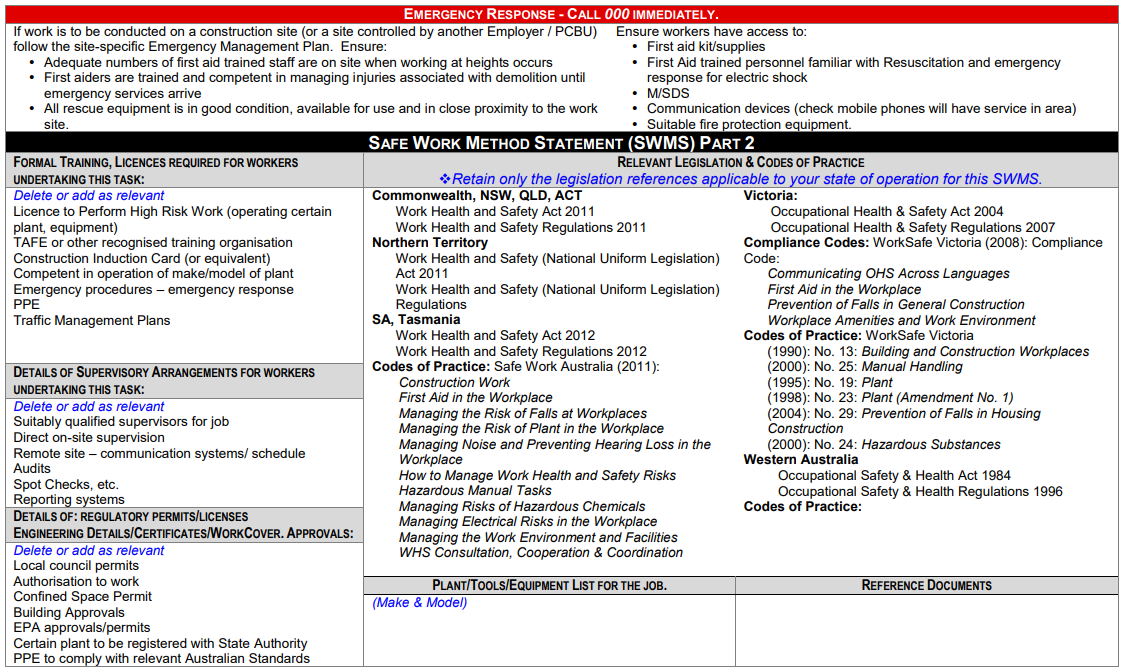
SWMS PART 2
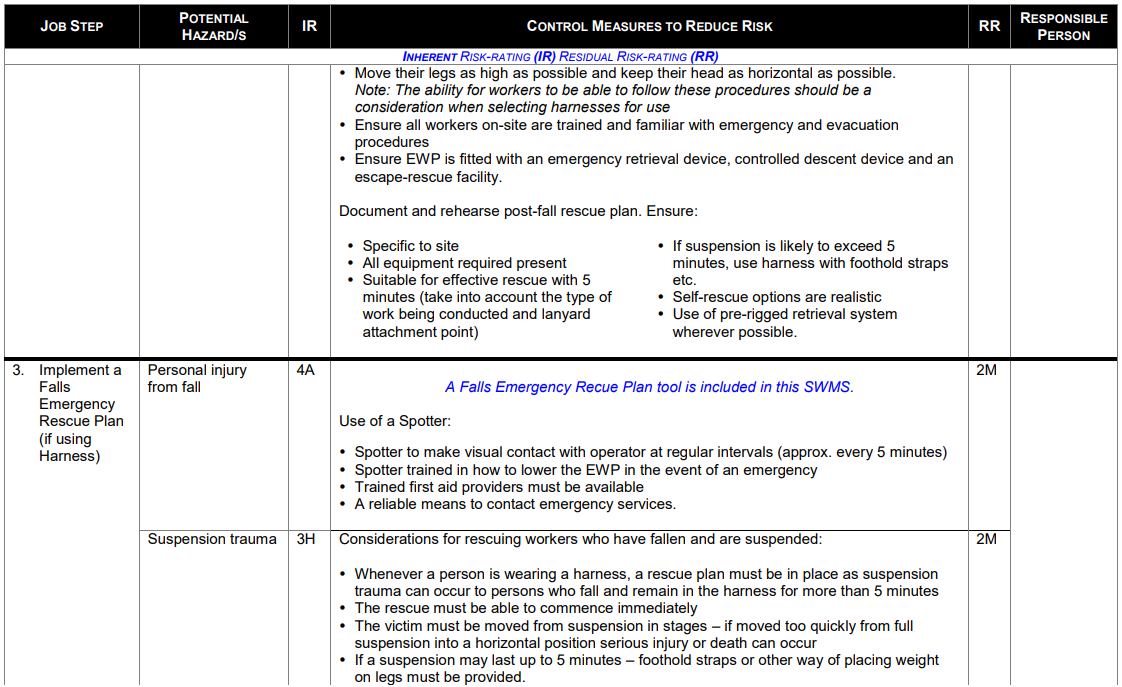

FALLS EMERGENCY RESCUE PLAN
-
Location of closest medical facility:
-
Approximate response time:
-
Location of closest emergency services:
-
Approximate response time:
-
Can rescue be undertaken onsite by trained personnel?
-
Indicate rescue equipment that will be provided:
- Fibre rope (meets relevant standards)
- Karabiner (number required?)
- Rescue Knife
- Auto-stop Descender
- Triple Lock Karabiner
- Rescue stretcher
- Round sling
- Pre-rigged control descent device
- Recovery pole
- Other? (Specify)
-
Specify
-
Provide details of communication equipment that will be used:
-
Provide details of trained rescue personnel (trained within last 12 month period):
Personnel
-
Name
-
Course Name
-
Date of training
-
Provide details of trained first aiders (trained within last 12 month period):
First aider
-
Name
-
Course Name
-
Date of training
-
Documented rescue plan developed?
-
Documented rescue plan rehearsed?
-
Documented Rescue plan accessible on site?
-
SWMS PART 3
-
This SWMS has been developed in consultation and cooperation with employee/workers and relevant Employer/Persons Conducting Business or Undertaking (PCBU). I have read the above SWMS and I understand its contents. I confirm that I have the skills and training, including relevant certification to conduct the task as described. I agree to comply with safety requirements within this SWMS including risk control measures, safe work instructions and Personal Protective Equipment described.
-
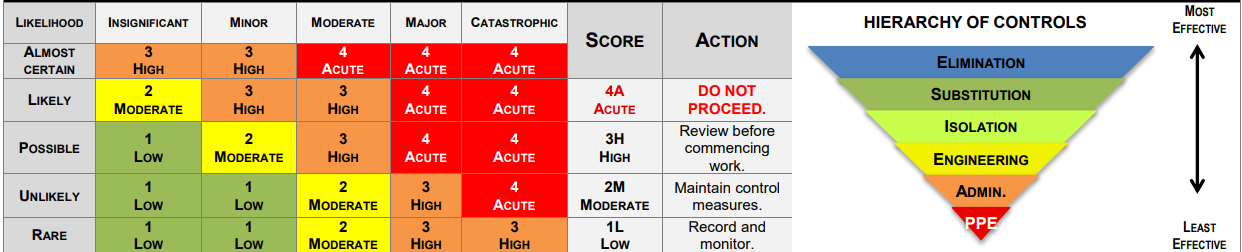
OVERALL RISK RATING AFTER CONTROLS: 2 MODERATE
EMPLOYEE/WORKER
-
EMPLOYEE/WORKER NAME AND SIGNATURE
-
JOB ROLE / POSITION
-
DATE AND TIME
-
EMPLOYER/PCBU/SUPERVISOR
REVIEW/MONITOR
-
REVIEW: Ensure all controls are reviewed as per the following:
- If controls fail to reduce risk adequately
- When changes to the workplace or work activity occur that create new / different risks where controls may no longer be effective
- New hazards identified
- After an incident involving work activities relevant to this SWMS
- During consultation with relevant persons indicate review is needed
- A Health and Safety Representative (HSR) requests a review in line with the requirements of the legislation. -
MONITOR: To ensure controls are implemented and monitored effectively:
- Toolbox /pre-work meetings will be undertaken
- Relevant persons will be consulted on hazards and contents of SWMS, work plans and other applicable information
- Control measures will be monitored throughout works:
* Spot checks * Consultation * Scheduled audits
- Corrective actions will be recorded and rectified in a timely manner SWMS will be reviewed and updated accordingly (in consultation with relevant persons)
REVIEW NO.
-
NAME AND SIGNATURE:
-
DATE:


