




Information
-
Incident Report & Investigation Form
-
Store Location
-
Type of Incident
-
Document No.
-
Conducted on
Reporting Details
-
Name of Person reporting the incident
-
Manager Name & Contact Number
- Khalil Abbas - Retail Operations Manager 0428 746 253
- Shaun Austen - Warehouse Operations Manager 0424 808 581
- Venkat Yenerni - Store Manager Crossroads 9083 6501
- Mark Mleczko - Store Manager - Blacktown 0448 478 066
- Anglela Hili - Administration Manager Blacktown 0405 219 939
- Ben Woods - Zone A Manager Blacktown 0405 219 939
- Debbie Contzonis - Furniture Supervisor Crossroads 0407 273 416
- Leyon Fereti - Flooring Supervisor Blacktown0402 247 249
- Craig Fisher - Warehouse Supervisor Blacktown 0431 454 868
- Kim Chamberlain - VM Manager 0409 257 413
- Jethro David - Zone B Manager Blacktown 0429 067 360
- Dinesh Sharma - Customer Service Supervisor Blacktown - 0451 531 660
-
Report Type
Injured Person Details
-
First Name
-
Surname
-
Date of Birth (dd/mm/yyyy)
-
Sex
-
Home Address
-
Contact Number
-
Which department do they work.
- Homewares
- Flooring
- Customer Service
- Furniture
- Bedding
- Kitchens
- Appliances
- Warehouse
- Support
- Visual Merchandising
- Not Applicable - Customer
- Not Applicable - Contractor
- Other
Occupation/Job Title & Details
-
Position Held
- Manager
- Supervisor
- Cafe
- Customer Service
- Salesperson
- Storeman
- Support Office
- VM Assistant
-
Employment Type
-
Usual Hours
-
Normal hours of work
-
Training/Qualifications Held
Incident Details
-
Date and time of incident
-
Date and time incident was reported.
-
Task at time of incident
-
To whom was the incident reported?
-
Where did this occur?
- Homewares
- Flooring
- Customer Service
- Furniture
- Bedding
- Kitchens
- Appliances
- Warehouse
- Support
- Visual Merchandising
- Not Applicable - Customer
- Not Applicable - Contractor
- Other
-
Description of the incident/what happened
-
Photo's of injury or Incident scene
-
Add sketches (if needed)
-
Are there any witness(es)? If yes, provide name(s) and contact phone numbers
-
If yes - Enter details here
-
If this incident was a result of a Product, enter the I0 number, description and take a photo
-
Take photo of product
DETAILS OF INJURY, IF APPLICABLE
-
Was the worker required to cease work (eg stop work for the day) or likely to cease work?
-
Injury/Illness
- Bruise, graze, scratch
- Amputation
- Anxiety/stress
- Asphyxia
- Back pain
- Bump/blow
- Burn/scald
- Broken bones(s)/fracture
- Dislocation (without fracture)
- Cut/laceration
- Puncture/penetration injury
- Foreign body
- Crush injury
- Chemical burn
- Electric shock/burn
- Effects of smoke
- Fatal Injury
- Hernia
- Loss of sight (temp or perm.)
- Sprain/strain
- Other injury
- No apparent injury
- Unknown
- N/A
-
Side of Body
-
Severity of Injury
- No Treatment (and return to work)
- First Aid (and return to work)
- Professional Medical Treatment Required
- Restricted Work
- Absence from Work
- Major Injury (eg broken bones)
- Fatal
-
Part of Body - Select more than one if required
- Abdomen
- Ankle
- Arm
- Back
- Calf
- Chest
- Ear
- Elbow
- Eye
- Face
- Finger
- Foot
- Groin
- Hand
- Head
- Hip
- Internal
- Knee
- Leg
- Neck
- Lung
- Mouth
- Shoulder
- Thigh
- Toes
- Wrist
- N/A
-
Area
- Upper
- Lower
- Inner
- Outer
- Cheek
- Chin
- Forehead
- Jaw
- Nose
- Thumb
- Index finger
- Middle figits
- Sole
- Big toe
- Little toe
- Back of Hand
- Palm of Hand
- Front
- Back
- Lips
- Inside mouth
- Teeth
- Unknown
- N/A
TREATMENT
-
Was treatment given
- No treatment given
- Treatment offered but refused
- Yes, at scene
- Yes, at local first aid point
- Yes, at local GP surgery
- Yes, at hospital
-
When was treatment given?
-
Who provided the treatment
-
Detail any first-aid or medical treatment administered. (Provide names)
-
Nature of treatment
-
What happened after initial treatment?
- Return to Work
- Resumed normal activities
- Sent or taken to hospital
- Referred to Local GP (workcover)
- Referred to hospital
- Referred to own GP
- Sent or taken home
- Other
- Not known
Investigation
INVESTIGATION (to be conducted by Manager in consultation with relevant employee's)
-
Why did this occur?
Hazard Identification and Risk Assessment information
-
What hazards have you identified?
-
What could have potentially happened?
-
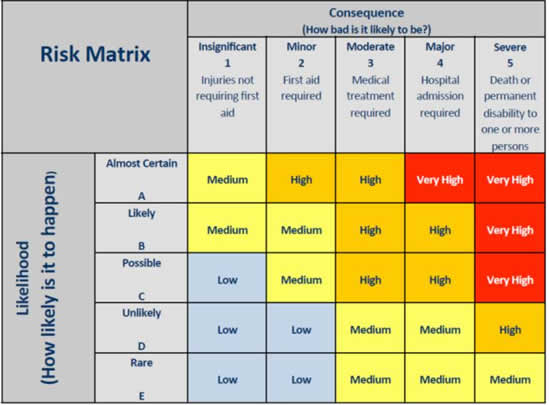
Likelihood (How likely is it to happen?)
-
Consequence (How bad is it likely to be)
-
Risk matrix
-
Name of Investigator
-
If not previously identified, enter the hazard and control implemented, onto the Risk register and allocate the same reference number for both forms for ease of cross referencing. If not effective, a Hazard Report Form is to be completed.
-
Using the Risk matrix, establish your rating
Hazard Control Strategy
-
Consider more than one control. the last two controls being the least effective
- Elimination
- Substitution
- Isolation
- Engineering
- Administrative
- PPE (Personal Protective Equipment)
-
If controlled immediately, list details here.
-
If longer term controls are required, list details here
-
Date to be implemented
Summary
-
Does the Manager believe that this hazard should be communicated with all employees?
-
If yes, how will this be communicated?
-
Date report completed
-
Manager confirms that consultation has been completed
-
Date
-
Employee representative verifies consultation has been complete
-
Date
-
Send this completed form within 24hrs of incident to injury@wngroup.com.au and your Store Manager


 - duplicate")