




Title Page
FJSA CORRECTIVE ACTION REQUEST
-
Section/Document Ref
-
Department:
-
CAR REF Number:
-
Responsible Person:
-
Auditor:
-
Date:
-
Details of Non-Conformance identified:
-
Confirmed By:
-
Signed:
-
Compliance Date:
Classification Of Finding:
-
Level 1 Constitutes non-compliance which necessitate the exercising of immediate discretionary enforcement action/powers vested in the inspectors, authorized officers and/or authorized persons in the interest of safeguarding aviation safety
-
Level 2 Constitutes non-compliance requiring the department to develop action plans with time frames and coupled with a follow-up inspection to verify rectification of the non-compliance
-
Level 3 Constitutes non-compliance which is left to the department to rectify and which will not necessitate a follow-up inspection but which can be followed up at the next inspection. The client is required to notify the CAA when the rectification has been effected within an agreed timeframe
Risk Matrix of Finding/If applicable:
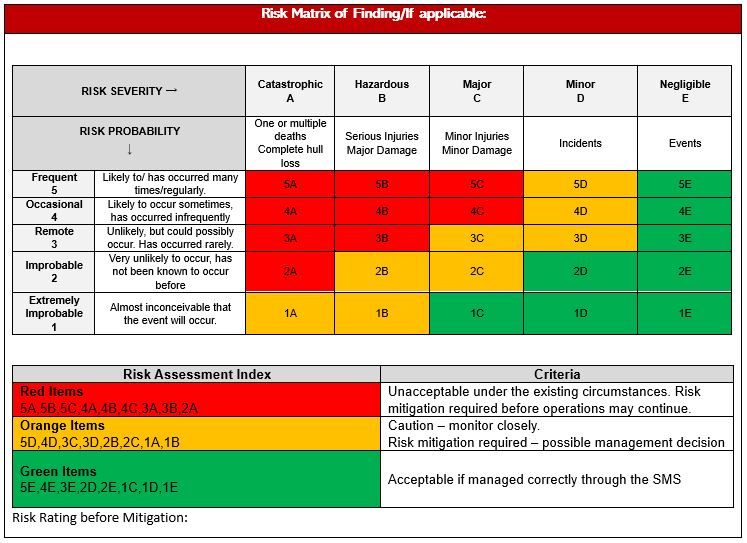
RISK RATING
-
Before CAP/ Mitigation:
-
After CAP/Mitigation:
Cause Category
-
1. Human Factors
-
2. Machine or Equipment
-
3. Management of tasks
-
4. Materials or parts
-
5. Medium/Work environment
-
6. Methods and Processes
Root Cause:
-
Complete the 5 WHY or SOAM Process
Root Cause of the Non-Conformance (5 WHY)
-
Five whys (5 whys) is a problem-solving method that explores the underlying cause-and-effect of particular problems. The primary goal is to determine the root cause of a defect or a problem by successively asking the question “Why?”.
-
1. WHY?
-
2. WHY?
-
3. WHY?
-
4. WHY?
-
5. WHY?
-
ROOT CAUSE:
-
The above table can be used for the 5 Why Root Cause analysis process. If required the SOAM process below can be used. Either process can be used depending on the complexity of the analysis.
ROOT CAUSE ANALYSIS (SOAM)
-
(Systemic Occurrence Analysis Methodology)
(Only complete the SOAM Analysis if the 5 Why process was not followed.) -
Step 1. Analyse Absent or Inadequate Controls:
The first step in analysing a hazard or occurrence involves identifying the protective controls (aka barriers or defences) that may have failed or been absent at the time of the occurrence. The existence of a hazard or occurrence indicates an absence of controls or, alternatively, that existing controls have been ineffective or inoperative. -
Awareness and understanding (prevention)
-
Restriction (prevention)
-
Detection (prevention/resolution)
-
Control and interim recovery (resolution)
-
Protection and containment (mitigation)
-
Escape and rescue (mitigation)
-
Awareness and understanding (prevention)
-
Step 2 – Analyse Human Involvement
The question for this stage should not be why people acted as they did, but simply what were their actions/inactions just prior to the event. This provides the starting point for the next stage of the analysis that focuses on trying to understand why people acted as they did, through examination of the contextual conditions in place at the time of the occurrence. The tasks performed by an operator involve various forms of information processing, including accurate detection, integration and interpretation of information, as well as planning, projecting and decision making. An information processing model is thus a logical component of an occurrence analysis methodology, enabling a comprehensive representation of the steps that might be performed by a controller as an abnormal event unfolds. The most effective remedial steps following a safety occurrence will be targeted at the barriers and contextual conditions that allowed the occurrence to take place. Nonetheless, in some circumstances it will be considered necessary to direct remedial efforts toward the errors that are identified using human factors techniques. In developing interventions to address human error it is ineffective to focus on changing human behaviour, as errors are part of being human and cannot be eliminated. Interventions are therefore most effective in reducing error if they are directed at the organisational- and system-level, and focus on addressing the contextual conditions that make it more likely that errors will occur. -
undefined
-
Step 3 - Analyse Contextual Conditions
Contextual conditions describe the circumstances that exist at the time of, or immediately prior to the safety occurrence. Originally described by Reason as “Psychological precursors of Unsafe Acts”, they have also been variously described as preconditions for unsafe acts, task and environmental conditions, situational factors, conditions, or performance shaping factors. As suggested by Reason’s original term (psychological precursors of unsafe acts), contextual conditions have the potential to exert a direct and powerful influence on human behaviour. they create an environment that may pre-dispose people to make errors and violations of the type described above. Hollnagel supports this view by suggesting that “actions at the sharp end” cannot be understood at all without reference to the condition of the people involved, their workplace, tools and equipment, and the organisation in which they work. -
Workplace conditions
-
Organisational climate
-
Attitudes and personality
-
Human performance limitations
-
Physiological and emotional factors
-
Workplace conditions
-
Step 4 - Analyse Organisational Factors
Organisational factors describe circumstances that pre-existed the occurrence and produced or allowed the existence of contextual conditions, which in turn influenced the actions and/or inactions of personnel. A total of 12 organisational risk factors (ORFs) have been identified as those that frequently contribute to safety occurrences, namely: -
Training
-
Workforce management
-
Accountability
-
Communication
-
Organisational culture
-
Competing goals
-
Policies and procedures
-
Maintenance management
-
Equipment and infrastructure
-
Risk management
-
Change management
-
External environment
-
Training
-
Additional Comments:
-
ROOT CAUSE:
-
NB: ORA's are, typically, the root causes that permit occurrences or the existence of hazards. Self-criticism is encouraged in order to identify the true nature of causal factors
Please complete the Corrective action plan and Root Cause in the required blocks on Page 3 of this form once the SOAM is completed
Please complete either the 5 Why process or the SOAM as required but not both.
Please complete the final Root Cause
Corrective Action Plan including mitigation actions required.
-
Short Term
-
Target Date:
-
Action Taken By:
-
Long Term
-
Target Date:
-
Action Taken By:
-
Add signature
QA/Safety Department: Acceptance of Corrective Action and Comments
-
Comments
-
Accepted/Approved By
Hazard Report Ref if applicable:
-
Refference
Follow Up
-
Follow Up Required:
-
Follow-Up Audit Type
-
Status/Progress/Re-evaluation:
-
QAM Signature
-
Department Head Signature







