




Title Page
-
Site conducted
-
Conducted on
-
Prepared by
-
Reference number
-
Incident Summary
Accident report
Incident Category:
-
What is the loss category?
-
Incident definitions
-
What is the accident category?
- Minor
- Major
- RIDDOR/RADOR
- Colleague illness (not work related accident)
-
Has this accident, or one similar to it, occurred on site within the last 30 days?
-
This accident requires a level two investigation
Define Problem
-
When was the accident?
-
Where did the accident occour in the facility?
-
What equipment was involved in the accident (include photo)
- Blade/ Knife
- Compactors
- Contractor owned equipment
- Customer product
- Dangerous Goods Item
- Display Screen Equipment
- Dock Leveller
- External Building damage
- Fire Equipment (extinguishers, alarms, lights, sounders)
- Hand tools (not including blades)
- Internal Buidling damage
- Manual Handling aids (trolleys, skates, hooks etc)
- MHE ( FLT, PPR, Wave, Turret etc)
- Office Seating
- Other
- Packaging material
- Pallets
- Racking
- Road Van/ Truck (Contractor owned)
- Road Van/ k (DBS owned)
- Roller Shutter door
- Waste
-
Please describe equipment involved
-
Who was the injured person (please use initials only)
-
What is their employment status?
-
What is their shift pattern?
-
Where on the body was their injury?
- Left side of body
- Right side of body
-
Where specifically on the left side of the body?
- Head
- Face
- Ear/ hearing
- Eye
- Nose
- Mouth
- Neck
- Shoulder
- Arm
- Elbow
- Wrist
- Hand
- Finger
- Torso (inc back injury)
- Hips
- Buttocks
- Thigh
- Knee
- Calf
- Ankle
- Foot
- Toes
-
all head injuries will require a full investigation
-
Circle the body part affected
-
Where specifically on the right side of the body?
- Head
- Face
- Ear/ hearing
- Eye
- Nose
- Mouth
- Neck
- Shoulder
- Arm
- Elbow
- Wrist
- Hand
- Finger
- Torso (inc back injury)
- Hips
- Buttocks
- Thigh
- Knee
- Calf
- Ankle
- Foot
- Toes
-
all head injuries will require a full investigation
-
Circle the body part affected
-
What was the injury type?
- Cut
- Abrasion
- Pain
- Bruising
- Sprain
- Stab
- Burn / Scald
- Fracture
- Crush
- Non-Injury i.e. feeling faint or nausea
-
Is this occurrence related to a previously known medical condition or injury?
-
Has this person received training in the task where the accident occurred?
-
Provide evidence of training such as certificate or attendance record
-
What level of experience does this person have?
-
Please describe the accident in detail
-
Was PPE required to be worn?
-
Which PPE was required to be worn?
- Hard hat/ bump cap
- Hearing protection
- Eye protection
- Respiratory equipment
- Hand protection
- Hi-Vis clothing
- Safety footwear
- Fall arrest kit/ Harness
-
Was the correct PPE being worn at the time of the accident?
-
Does CCTV or video footage exist of the accident?
-
Provide link to the footage or still screen shots
-
What was the immediate response?
- First Aid
- Quarantined the area/ equipment
- Walk-in center/ taken to A&E
- Communication to effected parties
-
Who was the first aider? (please use initials only)
-
Was treatment permitted?
-
What first aid treatment was applied?
- Pressure/ elevation to stop bleeding
- Cleaning of wound
- Application of dressing
- Control of the accident area
- Calling emergency services
- Other
-
Please specify first aid treatment applied
-
What time were the emergency services called?
-
What time did the emergency services arrive?
-
Were any witness statements documented?
-
Please attach the documents
-
Was Violence or Aggression involved?
-
The HR department must be involved
Completion
-
Name of person completing report
Designate Team
-
Team Leader:
-
Team Members:
Define Problem
-
When was the accident?
-
Where did the accident occour in the facility?
-
What equipment was involved in the accident (include photo)
- Blade/ Knife
- Compactors
- Contractor owned equipment
- Customer product
- Dangerous Goods Item
- Display Screen Equipment
- Dock Leveller
- External Building damage
- Fire Equipment (extinguishers, alarms, lights, sounders)
- Hand tools (not including blades)
- Internal Buidling damage
- Manual Handling aids (trolleys, skates, hooks etc)
- MHE ( FLT, PPR, Wave, Turret etc)
- Office Seating
- Other
- Packaging material
- Pallets
- Racking
- Road Van/ Truck (Contractor owned)
- Road Van/ k (DBS owned)
- Roller Shutter door
- Waste
-
Please describe equipment involved
-
Who was the injured person (please use initials only)
-
What is their employment status?
-
What is their shift pattern?
-
Where on the body was their injury?
- Left side of body
- Right side of body
-
Where specifically on the left side of the body?
- Head
- Face
- Ear/ hearing
- Eye
- Nose
- Mouth
- Neck
- Shoulder
- Arm
- Elbow
- Wrist
- Hand
- Finger
- Torso (inc back injury)
- Hips
- Buttocks
- Thigh
- Knee
- Calf
- Ankle
- Foot
- Toes
-
all head injuries will require a full investigation
-
Circle the body part affected
-
Where specifically on the right side of the body?
- Head
- Face
- Ear/ hearing
- Eye
- Nose
- Mouth
- Neck
- Shoulder
- Arm
- Elbow
- Wrist
- Hand
- Finger
- Torso (inc back injury)
- Hips
- Buttocks
- Thigh
- Knee
- Calf
- Ankle
- Foot
- Toes
-
all head injuries will require a full investigation
-
Circle the body part affected
-
What was the injury type?
- Cut
- Abrasion
- Pain
- Bruising
- Sprain
- Stab
- Burn / Scald
- Fracture
- Crush
- Non-Injury i.e. feeling faint or nausea
-
Is this occurrence related to a previously known medical condition or injury?
-
Has this person received training in the task where the accident occurred?
-
Provide evidence of training such as certificate or attendance record
-
What level of experience does this person have?
-
Please describe the accident in detail
-
Was PPE required to be worn?
-
Which PPE was required to be worn?
- Hard hat/ bump cap
- Hearing protection
- Eye protection
- Respiratory equipment
- Hand protection
- Hi-Vis clothing
- Safety footwear
- Fall arrest kit/ Harness
-
Was the correct PPE being worn at the time of the accident?
-
Does CCTV or video footage exist of the accident?
-
Provide link to the footage or still screen shots
-
What was the immediate response?
- First Aid
- Quarantined the area/ equipment
- Walk-in center/ taken to A&E
- Communication to effected parties
-
Who was the first aider? (please use initials only)
-
Was treatment permitted?
-
What first aid treatment was applied?
- Pressure/ elevation to stop bleeding
- Cleaning of wound
- Application of dressing
- Control of the accident area
- Calling emergency services
- Other
-
Please specify first aid treatment applied
-
What time were the emergency services called?
-
What time did the emergency services arrive?
-
Were any witness statements documented?
-
Please attach the documents
-
Was Violence or Aggression involved?
-
The HR department must be involved
-
Level One investigation is required
Designate Team
-
Team Leader:
Team Members:
-
Name of team member
Define Problem
-
When was the accident?
-
Where did the accident occour in the facility?
-
What equipment was involved in the accident (include photo)
- Blade/ Knife
- Compactors
- Contractor owned equipment
- Customer product
- Dangerous Goods Item
- Display Screen Equipment
- Dock Leveller
- External Building damage
- Fire Equipment (extinguishers, alarms, lights, sounders)
- Hand tools (not including blades)
- Internal Buidling damage
- Manual Handling aids (trolleys, skates, hooks etc)
- MHE ( FLT, PPR, Wave, Turret etc)
- Office Seating
- Other
- Packaging material
- Pallets
- Racking
- Road Van/ Truck (Contractor owned)
- Road Van/ k (DBS owned)
- Roller Shutter door
- Waste
-
Please describe equipment involved
-
Who was the injured person (please use initials only)
-
What is their employment status?
-
What is their shift pattern?
-
Where on the body was their injury?
- Left side of body
- Right side of body
-
Where specifically on the left side of the body?
- Head
- Face
- Ear/ hearing
- Eye
- Nose
- Mouth
- Neck
- Shoulder
- Arm
- Elbow
- Wrist
- Hand
- Finger
- Torso (inc back injury)
- Hips
- Buttocks
- Thigh
- Knee
- Calf
- Ankle
- Foot
- Toes
-
all head injuries will require a full investigation
-
Circle the body part affected
-
Where specifically on the right side of the body?
- Head
- Face
- Ear/ hearing
- Eye
- Nose
- Mouth
- Neck
- Shoulder
- Arm
- Elbow
- Wrist
- Hand
- Finger
- Torso (inc back injury)
- Hips
- Buttocks
- Thigh
- Knee
- Calf
- Ankle
- Foot
- Toes
-
all head injuries will require a full investigation
-
Circle the body part affected
-
What was the injury type?
- Cut
- Abrasion
- Pain
- Bruising
- Sprain
- Stab
- Burn / Scald
- Fracture
- Crush
- Non-Injury i.e. feeling faint or nausea
-
Is this occurrence related to a previously known medical condition or injury?
-
Has this person received training in the task where the accident occurred?
-
Provide evidence of training such as certificate or attendance record
-
What level of experience does this person have?
-
Please describe the accident in detail
-
Was PPE required to be worn?
-
Which PPE was required to be worn?
- Hard hat/ bump cap
- Hearing protection
- Eye protection
- Respiratory equipment
- Hand protection
- Hi-Vis clothing
- Safety footwear
- Fall arrest kit/ Harness
-
Was the correct PPE being worn at the time of the accident?
-
What were the environmental conditions at the time of the accident?
- Sunny
- Raining
- Windy
- Overcast
- Snow/ Ice
- Extreme heat
-
Does CCTV or video footage exist of the accident?
-
Provide link to the footage or still screen shots
-
What was the immediate response?
- First Aid
- Quarantined the area/ equipment
- Walk-in center/ taken to A&E
- Communication to effected parties
-
Who was the first aider? (please use initials only)
-
Was treatment permitted?
-
What first aid treatment was applied?
- Pressure/ elevation to stop bleeding
- Cleaning of wound
- Application of dressing
- Control of the accident area
- Calling emergency services
- Other
-
Please specify first aid treatment applied
-
What time were the emergency services called?
-
What time did the emergency services arrive?
-
Were any witness statements documented?
-
Please attach the documents
-
Was Violence or Aggression involved?
-
The HR department must be involved
-
RIDDOR Category
- Specified Injury
- Over Seven Day Incapacitation of a worker
- (ROI ONLY) Over Three Day Incapacitation of a worker
- Reportable Disease
- Dangerous Occurrence
- Injury to Non-Worker i.e. Visitor or Member of Public
-
RIDDOR Website England/ Scotland/ Wales: https://www.hse.gov.uk/riddor/report.htm
-
RIDDOR Website Northern Ireland: https://www.hseni.gov.uk/report-incident
-
RADOR Website ROI: https://webapps.hsa.ie/Account/Login?ReturnUrl=%2f
-
RIDDOR / RADOR Reference Number (attach a copy of the report to this pack)
-
Who made the RIDDOR / RADOR report? (print name)
-
This incident does not require an investigation
-
When was the incident?
-
Where did the incident occur in the facility?
-
Who was involved (please use initials only)
-
What is their employment status?
-
Describe the incident
-
What treatment was given?
- First Aid
- Quarantined the area/ equipment
- Walk-in center/ taken to A&E
- Communication to effected parties
-
Who was the first aider? (please use initials only)
-
Has their manager been informed?
Sign off
-
Name of person reporting incident
-
Incident definitions
-
What is the environmental incident category?
- Minor
- Major
- RIDDOR/RADOR
- Colleague illness (not work related accident)
Investigation Team
-
Team leader
Team Members
-
Name of Team member
Define Problem
-
When was the incident.
-
Where did the incident occur
- Warehouse
- Office
- Yard
- Offsite
- Whole Facility
-
What equipment/infrastructure/products/services/scenario involved.
-
What was the cause of the chemical spill
- Loss of vehicle fuel containment
- Damaged chemical container
- Incorrect use of chemical
- During decanting process
-
Description of the incident in detail
-
What was your immediate response
- Access to site checked/made secure
- Air Con/heating switched off/windows closed.
- Alarm Raised (External)
- Alarm Raised (Internal System)
- Absorbent socks used to prevent spread
- Area cleared of excess water
- Area cleared of litter/dirt
- Bin/Skip covered/sealed
- Building Evacuated
- Customer stock removed from the area.
- Drains blocked with drain covers
- Doors closed in warehouse/temperature controlled areas.
- Equipment and machinery removed from the area.
- Equipment serviced/calibrated.
- Fire fighting/suppression equipment ordered/distributed.
- Fire tackled
- Leak plugged/sealed
- Leaking drum/vessel placed on bunded pallet
- Main site shut off taps closed.
- Nothing
- Spill kit and/or consumables ordered/distributed.
- Storage/spill bund drained of water.
- Storage/spill bund protected against weather
- Unused electrical devices turned off.
- Waste removed and placed in correct bins/skips
- Waste stored elsewhere (Temporary)
- Water outlets turned off
- Weeping/dripping valves/pipes repaired.
- Other
-
Who was involved (Use initials only)
-
What is their employment status?
-
Has this person received training in the task where the accident occurred?
-
Provide evidence of training such as certificate or attendance record
-
What level of experience does this person have?
-
Please describe the accident in detail
-
Does CCTV or video footage exist of the accident?
-
Provide link to the footage or still screen shots
-
Did anyone witness the event?
-
Was a written witness statement(s) taken from the individuals?
-
Attach witness statement to the report here.
-
What was the cause of the waste issue
-
Who was involved (Use initials only)
-
What was the immediate response.
-
Description of the incident in detail
-
Did anyone witness the incident
-
Was a written statement(s) taken from the individuals?
-
Attach statement(s) here
-
Take statement(s) and attach here
-
What was the cause of the utility issue.
- Combination of gas heating, air conditioning or open doors/windows working against each other.
- Electrical machinery/devices left on for excessive periods/overnight when not in use.
- Gas heating systems left on or not moved to tick-over mode when office unoccupied during the evening/weekend.
- Warehouse heating/temperature control systems left on with doors/shutters left open.
- Water outlets for cleaning, vehicle washing or welfare left running unnecessarily.
- Fluid/Fuel leak of a vehicle/plant/tank (3rd party owned)
- Fluid/Fuel leak of a vehicle/plant/tank (DBS Owned)
- Leak from customer owned goods
- Drainage system failure
- Gutting overflowing
- Office flooded - Unable to operate
- Office flooded - Able to operate but with distruptions
- Roof leaking
- Weather damage to doors, gates, roof walls and/or windows
- Yard flooded - Unable to operate
- Yard flooded - Able to operate but with disruptions.
- Arson/deliberate act.
- Carelessness by individual (E.g. discarded smoking materials).
- Electrical fault (fixed wiring)
- Issues during repairs/modifications to equipment/facility (3rd Party Contractors)
- Reactions from hazardous materials
- Stand alone office/warehouse devices creating fumes, overheating or smoking.
- Electrical fault (cables/equipment).
- Extreme wet/windy weather/storm
- Burst Pipes
- Taps/water outlets left running
-
Who was involved (Use initials only)
-
What was the immediate response (ADD DETAILED DROPDOWN)
-
Description of the incident in detail
-
Did anyone witness the event.
-
Was a written witness statement(s) taken from the individual
-
Attach statement(s) here.
-
Take statement(s) and attach to the report here.
-
What was the cause of the fire.
-
Description of the incident in detail
-
What was the immediate response.
-
Did anyone witness the event
-
Was a written witness statement(s) taken from the individuals?
-
Attach the witness statement(s) here.
-
Take statement(s) and attach to the report here.
-
What was the cause of the fire.
-
Who was involved (Use initials only).
-
Description of the incident in detail
-
What was the immediate response
-
Did anyone witness the event
-
Was a written witness statement(s) taken from the individual(s)?
-
Take statements from the individual(s) and attach to the report here.
-
Attach the statement(s) to the incident report here.
-
What was the result of the flood or weather event?
-
The line manager is responsible for completing the online form https://www.gov.uk/report-an-environmental-incident (UK) / https://www.epa.ie/ (IRE). Support can be obtained from the QSHE team qshe@dbschenker.com and must inform their senior manager of the accident as soon as possible.
-
Has this incident, or one similar to it, occurred on site within the last 30 days
-
This incident requires a level one investigation
Investigation Team
-
Team leader
Team Members
-
Name of Team member
Define Problem
-
When was the incident.
-
Where did the incident occur
- Warehouse
- Office
- Yard
- Offsite
- Whole Facility
-
What equipment/infrastructure/products/services/scenario involved.
-
What was the cause of the chemical spill
- Loss of vehicle fuel containment
- Damaged chemical container
- Incorrect use of chemical
- During decanting process
-
Description of the incident in detail
-
What was your immediate response
- Access to site checked/made secure
- Air Con/heating switched off/windows closed.
- Alarm Raised (External)
- Alarm Raised (Internal System)
- Absorbent socks used to prevent spread
- Area cleared of excess water
- Area cleared of litter/dirt
- Bin/Skip covered/sealed
- Building Evacuated
- Customer stock removed from the area.
- Drains blocked with drain covers
- Doors closed in warehouse/temperature controlled areas.
- Equipment and machinery removed from the area.
- Equipment serviced/calibrated.
- Fire fighting/suppression equipment ordered/distributed.
- Fire tackled
- Leak plugged/sealed
- Leaking drum/vessel placed on bunded pallet
- Main site shut off taps closed.
- Nothing
- Spill kit and/or consumables ordered/distributed.
- Storage/spill bund drained of water.
- Storage/spill bund protected against weather
- Unused electrical devices turned off.
- Waste removed and placed in correct bins/skips
- Waste stored elsewhere (Temporary)
- Water outlets turned off
- Weeping/dripping valves/pipes repaired.
- Other
-
Who was involved (Use initials only)
-
What is their employment status?
-
Has this person received training in the task where the accident occurred?
-
Provide evidence of training such as certificate or attendance record
-
What level of experience does this person have?
-
Please describe the accident in detail
-
Does CCTV or video footage exist of the accident?
-
Provide link to the footage or still screen shots
-
Did anyone witness the event?
-
Was a written witness statement(s) taken from the individuals?
-
Attach witness statement to the report here.
-
What was the cause of the waste issue
-
Who was involved (Use initials only)
-
What was the immediate response.
-
Description of the incident in detail
-
Did anyone witness the incident
-
Was a written statement(s) taken from the individuals?
-
Attach statement(s) here
-
Take statement(s) and attach here
-
What was the cause of the utility issue.
- Combination of gas heating, air conditioning or open doors/windows working against each other.
- Electrical machinery/devices left on for excessive periods/overnight when not in use.
- Gas heating systems left on or not moved to tick-over mode when office unoccupied during the evening/weekend.
- Warehouse heating/temperature control systems left on with doors/shutters left open.
- Water outlets for cleaning, vehicle washing or welfare left running unnecessarily.
- Fluid/Fuel leak of a vehicle/plant/tank (3rd party owned)
- Fluid/Fuel leak of a vehicle/plant/tank (DBS Owned)
- Leak from customer owned goods
- Drainage system failure
- Gutting overflowing
- Office flooded - Unable to operate
- Office flooded - Able to operate but with distruptions
- Roof leaking
- Weather damage to doors, gates, roof walls and/or windows
- Yard flooded - Unable to operate
- Yard flooded - Able to operate but with disruptions.
- Arson/deliberate act.
- Carelessness by individual (E.g. discarded smoking materials).
- Electrical fault (fixed wiring)
- Issues during repairs/modifications to equipment/facility (3rd Party Contractors)
- Reactions from hazardous materials
- Stand alone office/warehouse devices creating fumes, overheating or smoking.
- Electrical fault (cables/equipment).
- Extreme wet/windy weather/storm
- Burst Pipes
- Taps/water outlets left running
-
Who was involved (Use initials only)
-
What was the immediate response (ADD DETAILED DROPDOWN)
-
Description of the incident in detail
-
Did anyone witness the event.
-
Was a written witness statement(s) taken from the individual
-
Attach statement(s) here.
-
Take statement(s) and attach to the report here.
-
What was the cause of the fire.
-
Description of the incident in detail
-
What was the immediate response.
-
Did anyone witness the event
-
Was a written witness statement(s) taken from the individuals?
-
Attach the witness statement(s) here.
-
Take statement(s) and attach to the report here.
-
What was the cause of the fire.
-
Who was involved (Use initials only).
-
Description of the incident in detail
-
What was the immediate response
-
Did anyone witness the event
-
Was a written witness statement(s) taken from the individual(s)?
-
Take statements from the individual(s) and attach to the report here.
-
Attach the statement(s) to the incident report here.
-
What was the result of the flood or weather event?
-
This accident requires a level two investigation
-
When was the accident?
-
Where did the accident occour in the facility?
-
What equipment was involved in the accident (include photo)
- Blade/ Knife
- Compactors
- Contractor owned equipment
- Customer product
- Dangerous Goods Item
- Display Screen Equipment
- Dock Leveller
- External Building damage
- Fire Equipment (extinguishers, alarms, lights, sounders)
- Hand tools (not including blades)
- Internal Buidling damage
- Manual Handling aids (trolleys, skates, hooks etc)
- MHE ( FLT, PPR, Wave, Turret etc)
- Office Seating
- Other
- Packaging material
- Pallets
- Racking
- Road Van/ Truck (Contractor owned)
- Road Van/ k (DBS owned)
- Roller Shutter door
- Waste
-
Please describe equipment involved
-
Who was involved (please use initials only)
-
What is their employment status?
-
Has this person received training in the task where the accident occurred?
-
Provide evidence of training such as certificate or attendance record
-
What level of experience does this person have?
-
Please describe the accident in detail
-
Does CCTV or video footage exist of the accident?
-
Provide link in the notes to the location of the footage or still screen shots
-
What was the immediate response?
- First Aid
- Quarantined the area/ equipment
- Walk-in center/ taken to A&E
- Communication to effected parties
-
Who was the first aider? (please use initials only)
-
Were any witness statements documented?
-
Please attach the documents
-
Obtain witness statements from the injured person, first aiders and any witnesses.
-
Does a risk assessment exist for this task?
-
Has the risk assessment been reviewed?
-
The risk assessment must be reviewed before closing this investigation
-
What is the risk assessment reference?
-
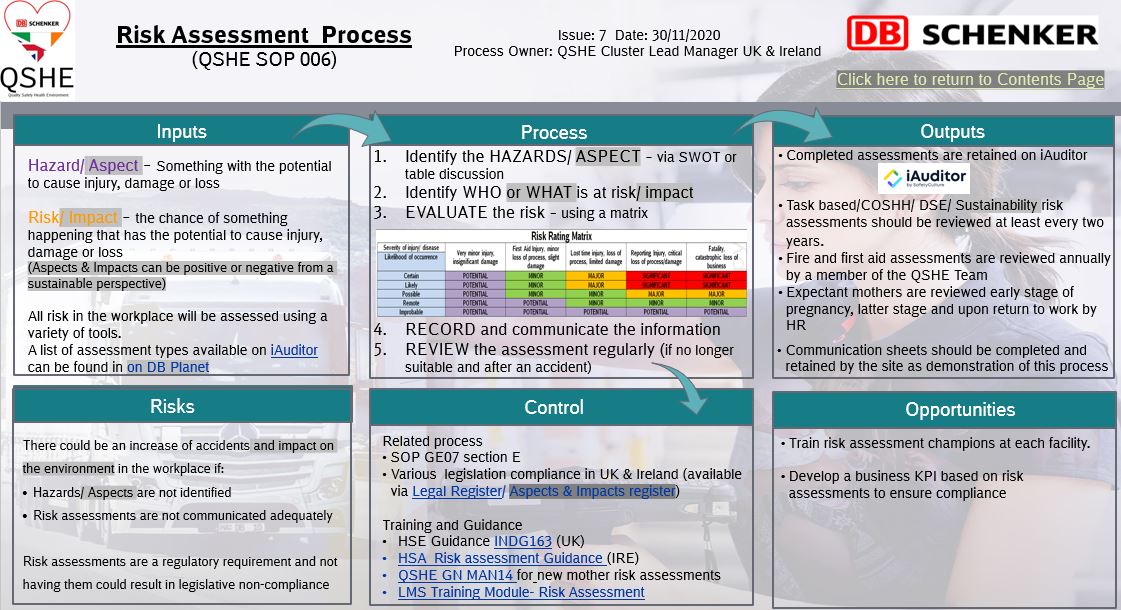
A risk assessment must be devised and communicated. Please raise an action to complete an assessment as required in QSHE SOP 006
-
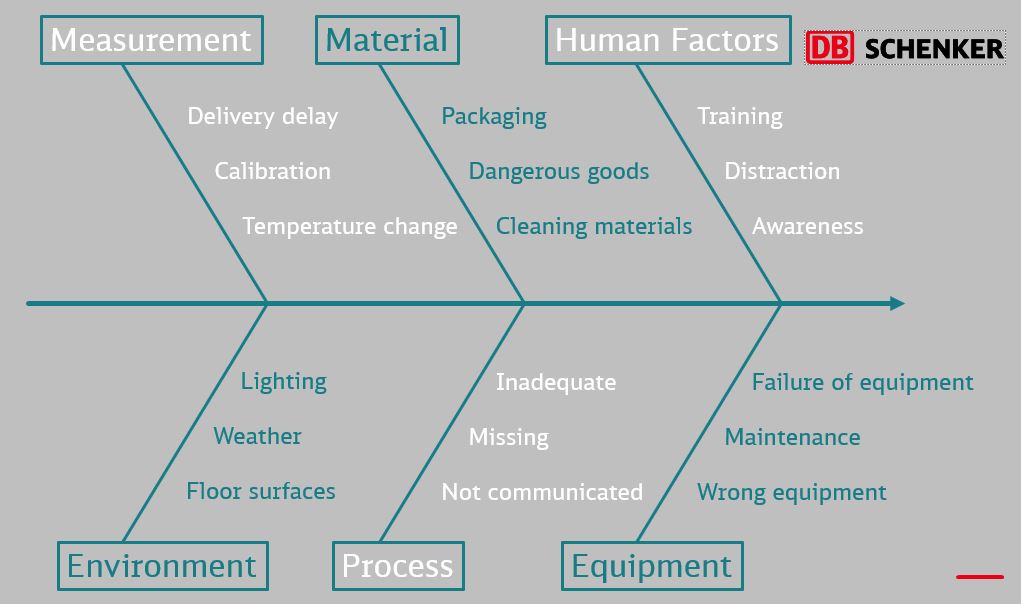
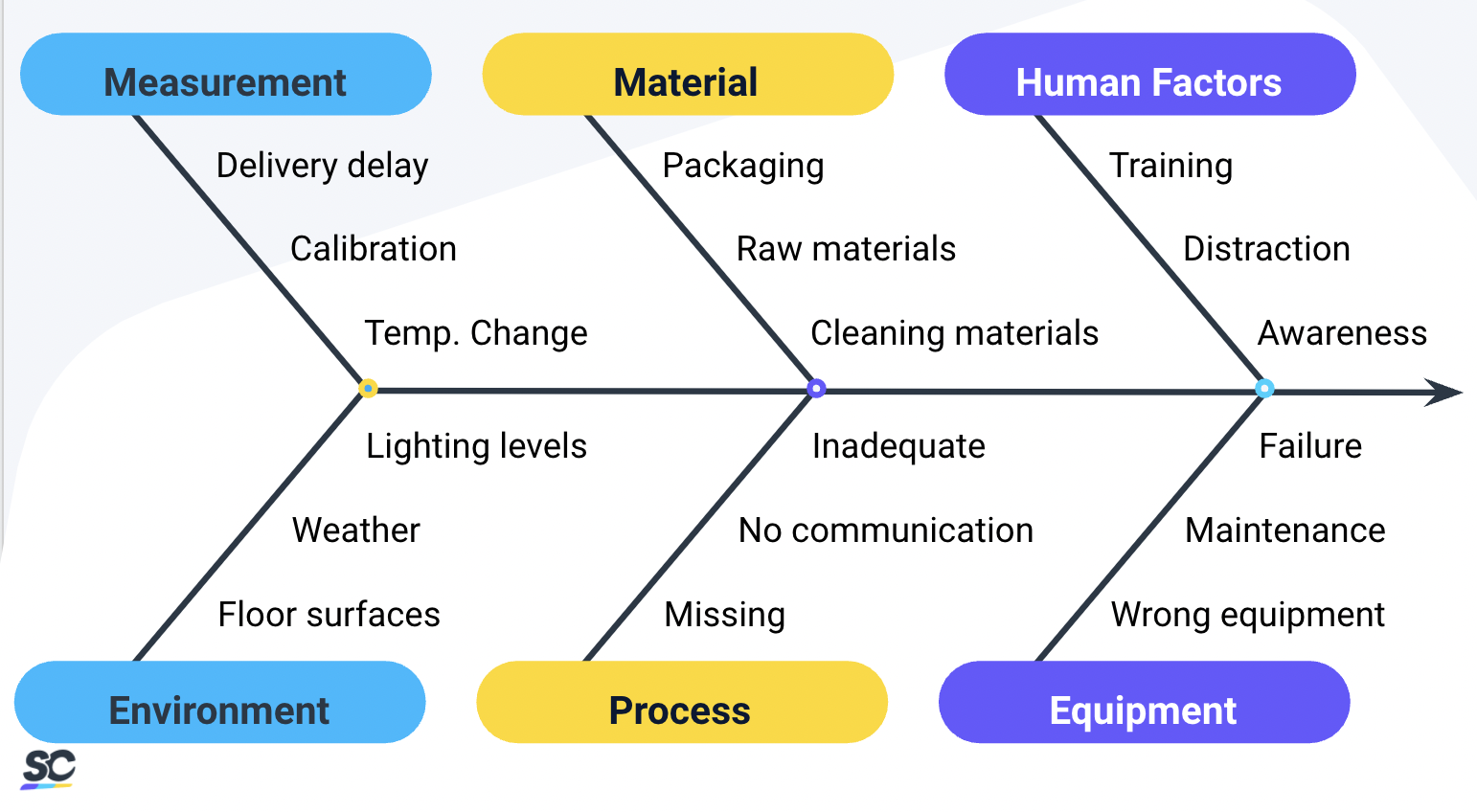
For a level 2 investigation we use a simple Ishikawa principle to determine a potential root cause
-
What was the potential cause of this accident?
- Human factors
- Materials
- Measurement
- Equipment
- Process
- Environment
-
What corrective actions have been implemented to improve the human factor cause of this accident?
- Lessons Learnt communicated
- Re-trianing
- Other
-
Please describe the action implemented
-
Has this action been completed?
-
The investigation can not be closed until the action is completed
-
Provide evidence of the completed action
-
Has this action been completed?
-
Has this action been completed?
-
What corrective actions have been implemented to improve the materials used in this accident? (include details in the notes)
- New supplier
- Improved materials
- Other
-
Please describe the action implemented
-
Has this action been completed?
-
Has this action been completed?
-
Has this action been completed?
-
What corrective actions have been implemented to improve the measurement aspects of this accident? (include details in the notes)
- Re-calibration
- Delays managed
- Other
-
Please describe the action implemented
-
Has this action been completed?
-
Has this action been completed?
-
Describe corrective action implemented
-
Has this action been completed?
-
What corrective actions have been implemented to improve the equipment used in this accident? (include details in the notes)
- Fixed equipment
- Quarantined equipment
- Disposed of equipment
- Other
-
Please describe the action implemented
-
Has this action been completed?
-
Has this action been completed?
-
Describe the action required to improve the equipment used in the accident
-
Has this action been completed?
-
Has this action been completed?
-
What corrective actions have been implemented to improve the process related to this accident? (include details in the notes)
- Process reviewed
- Process written
- Other
-
Please describe the action implemented
-
Has this action been completed?
-
Has this action been completed?
-
Has this action been completed?
-
What corrective actions have been implemented to improve the environment associated with this accident? (include details in the notes)
- Improved waste management
- Additional spill equipment
- Controlled work area
- Other
-
Has this action been completed?
-
Has this action been completed?
-
Has this action been completed?
-
Has this action been completed?
Completion
-
Name of person completing report
Investigation of Accident
Interim Containment
-
Describe what has been put in place to stop the issue from escalating?
- Human factors
- Materials
- Measurement
- Equipment
- Process
- Environment
-
What corrective actions have been implemented to improve the human factor cause of this accident?
- Lessons Learnt communicated
- Re-trianing
- Other
-
Please describe the action implemented
-
Has this action been completed?
-
Has this action been completed?
-
Has this action been completed?
-
What corrective actions have been implemented to improve the materials used in this accident?
- New supplier
- Improved materials
- Other
-
Please describe the action implemented
-
Has this action been completed?
-
Has this action been completed?
-
Has this action been completed?
-
What corrective actions have been implemented to improve the measurement aspects of this accident?
- Re-calibration
- Delays managed
- Other
-
Please describe the action implemented
-
Has this action been completed?
-
Has this action been completed?
-
Describe corrective action implemented
-
Has this action been completed?
-
What corrective actions have been implemented to improve the equipment used in this accident?
- Fixed equipment
- Quarantined equipment
- Disposed of equipment
- Other
-
Please describe the action implemented
-
Has this action been completed?
-
Has this action been completed?
-
Describe the action required to improve the equipment used in the accident
-
Has this action been completed?
-
Has this action been completed?
-
What corrective actions have been implemented to improve the process related to this accident?
- Process reviewed
- Process written
- Other
-
Please describe the action implemented
-
Has this action been completed?
-
Has this action been completed?
-
Has this action been completed?
-
What corrective actions have been implemented to improve the environment associated with this accident?
- Improved waste management
- Additional spill equipment
- Controlled work area
- Other
-
Please describe the action implemented
-
Has this action been completed?
-
Has this action been completed?
-
Has this action been completed?
-
Has this action been completed?
Verify and Determine the root cause
-
You can use the simple Ishikawa principle to determine a potential root cause as a brain storming tool with the colleagues or the 5 Why process
-
Which root cause analysis will you use?
- 5 Why
- Ishikawa
- Other
5 Why Analysis (click the green + button to complete)
-
What is the problem you are going to root cause analyse
-
Why?
-
Why?
-
Why?
-
Why?
-
Why?
-
As determined by the 5Why above, what are the Immediate/Direct Causes (circumstances that immediately precede the accident)
- Slip
- Trip
- Stab / Puncture
- Cut / Laceration
- Lifting / Carrying
- Pushing / Pulling
- Fall (same level)
- Fall from height
- Unauthorised use of equipment
- Not wearing required PPE
- Not following training
- Struck by moving vehicle
- Equipment Fault or Failure
- Personal attack
- Contact with moving machinery
- Struck by falling / flying objects
- Contact with electricty
- Struck against fixed / stationary object
- Removal of safety guards
- Exposure / contact with harmful substance(s)
- Burns / Scalds from exposure to Fire or Heat
- Trap or Pinch
- Horseplay
- Non- Injury i.e. fainting, nose bleed, black out, rash, bee sting, etc.
-
As determined by the 5Why above, what is the Basic/Root Cause for the accident?
- Personal/ Human Factors
- Job/ System Factors
-
What was the Person/ Human Factor Root cause?
-
What is the job/ system factor of the root cause
Define and implement Corrective Actions (e.g what actions can be taken to rectify the root casues identified in section 4)
-
Include a Actions and assign a SMART objective
Verify Permanent Corrections (PCs) for Problem
-
Can the issue be recreated by removing one or more of the results identified in section 5?
-
Can the problem be corrected again by reinstating the results identified above?
Prevent Recurrence
-
Has the problem has reoccurred since implementation of all actions.
-
The root cause analysis should be reviewed and additional prevenatative actions implemented
-
Does a risk assessment exist for this task?
-
Has the risk assessment been reviewed?
-
The risk assessment must be reviewed before closing this investigation
-
What is the risk assessment reference?
-
A risk assessment must be devised and communicated. Please raise an action to complete an assessment as required in QSHE SOP 006
-
Has the procedure/ process been updated?
-
Have the results and improvements been communicated to all affected persons?
-
Has the corrective action been witnessed?
-
If the answer is yes to all of the above in this section, then the investigation is ready to be closed
Sign off
End of Investigation - Sign off
-
What time was lost due to the accident (mins/ hours/ days)?
-
Team Leader sign off:
-
First Aider sign off:
-
Completion Date






