Information
-
Document No.
-
Audit Title
-
Client / Site
-
Conducted on
-
Prepared by
-
Location
-
Personnel
Plan A: Initial tracheal intubation plan
-
Direct laryngoscopy
-
Check:
-
Neck flexion and head extension
-
Laryngoscope technique and vector
-
External laryngeal manipulation - by laryngoscopist
-
Vocal cords open and immobile
-
If poor view: Introducer (bougie) - seek clicks or hold-up and/or alternative laryngoscope
-
Succeed? <br>Not more than 4 attempts. Maintaining 1) oxygenation with face mask and 2) anaesthesia
-
Tracheal intubation
-
Tracheal intubation verified?<br>
-
How was tracheal intubation verified?
- visual
- capnograph
- oesophageal detector
-
Proceed with surgery
-
"If in doubt, take it out"
Plan B: Secondary tracheal intubation plan
-
ILMA or LMA
-
Succeed? <br>Not more than 2 insertions <br>Oxygenate and ventilate<br>
-
Confirm: Ventilation
-
Confirm: Oxygenation
-
Confirm: Anaesthesia
-
Confirm: CVS stability
-
Confirm: Muscle relaxation
-
Fibreoptic tracheal intubation through IMLA or LMA - 1 attempt
If LMA consider long flexometallic, nasal RAE or microlaryngeal tube -
Fibreoptic tracheal intubation through IMLA or LMA verified?
-
How was tracheal intubation verified?
- visual
- capnograph
- oesophageal detector
-
Proceed with surgery
-
Postpone surgery
Awaken patient
Plan C: Maintenance of oxygenation, ventilation, postponement of surgery and awakening
-
Revert to face mask
Oxygenate and ventilate
Reverse non-depolarising relaxant
1 or 2 person mask technique -
Succeed?
-
Postpone surgery
Awaken patient
Plan D: Rescue techniques for "can't intubate, can't ventilate" situation
-
LMA
-
Improved oxygenation?
-
Awaken patient
-
Cannula cricothyroidotomy or surgical cricothyroidotomy?
-
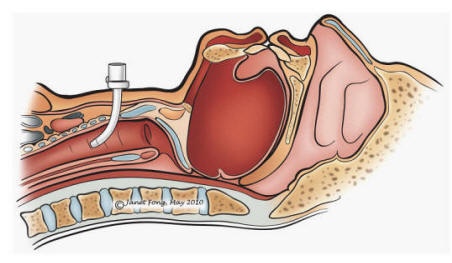
Cannula cricothyroidotomy
http://www.aic.cuhk.edu.hk/web8/dilational_cricothyrotomy.htm -
-
more information
-
Equipment: Kink-resistant cannula, e.g. Patil (Cook) or Ravussin (VBM), high-pressure ventilation system, e.g. Manujet III (VBM)
Technique:
1. Insert cannula through cricothyroid membrane
2. Maintain position of cannula - assistant's hand
3. Confirm tracheal position by air aspiration - 20ml syringe
4. Attach ventilation system to cannula
5. Commence cautious ventilation
6. Confirm ventilation of lungs and exhalation through upper airway
7. If ventilation fails or surgical emphysema or any other complication develops - convert immediately to surgical cricothyroidotomy -
Cannula cricothyroidotomy successful?
-
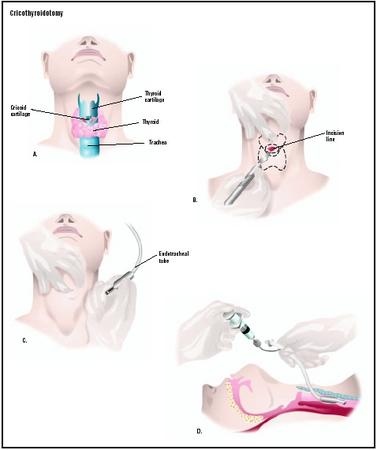
Surgical cricothyroidotomy
-
-
more information
-
Equipment: Scalpel - short and rounded (no. 20 or Minitrach scalpel), small (e.g. 6 or 7 mm) cuffed tracheal or tracheostomy tube
4-step technique:
1. Identify cricothyroid membrane
2. Stab incision through skin and membrane, enlarge incision with blunt dissection (e.g. scalpel handle, forceps or dilator)
3. Caudal traction on cricoid cartilage with tracheal hook
4. Insert tube and inflate cuff
Ventilate with low-pressure source
Verify tube position and pulmonary ventilation -
Surgical cricothyroidotomy
-
-
more information
-
Equipment: Scalpel - short and rounded (no. 20 or Minitrach scalpel), small (e.g. 6 or 7 mm) cuffed tracheal or tracheostomy tube
4-step technique:
1. Identify cricothyroid membrane
2. Stab incision through skin and membrane, enlarge incision with blunt dissection (e.g. scalpel handle, forceps or dilator)
3. Caudal traction on cricoid cartilage with tracheal hook
4. Insert tube and inflate cuff
Ventilate with low-pressure source
Verify tube position and pulmonary ventilation