




Information
-
Reference (Job number / DS1 / Date)
DELTA SERVICES Weekly Site Pack
-
-
Contract Title:
-
Address:
-
Supervisor:
-
Contract Manager:
-
Contract Number:
-
Week Number:
-
Date From:
-
Date To:

Contract Manager / Supervisor Pre - Start Checksheet
-
The following form must be filled in during the Pre Start Briefing / Site Visit by the manager responsible for the project
-
SITE DETAILS
Please include any details or corrective actions identified -
If notifiable has the project served its 14 day notice period?
-
Is the project starting on the planned date?
-
If the project has not started on the planned date, has the HSE been notified of delay to the start date in writing?
-
Has a copy of the email / notice sent to the HSE been given to the Supervisor / Foreman?
-
Is this the correct and most up to date version of the Method Statement on site?
-
Is there a copy of the ASB5, Licence and insurance on site?
-
Is the site set up and works as described in the Method Statement?
-
Is there at least one Waste Consignment Note on site?
-
How is the waste being removed from site?
-
Is it any different to that described in the Method Statement?
-
Is the DOP certification for all plant on site available and in date for the duration of the works?
-
Is the plant on site requiring PAT Electrical Testing labelled and on site?
-
Does the Supervisor / Foreman have Risk Assessment, CoSHH and Standard Procedures with him? Are they the current revisions?
-
For out of hours working, is security / client cover agreed?
-
Where a specialist plant is being used, is the team appropriately trained and a site specific risk assessment provided?
-
Has the client completed all isolations, provided all attendances agreed and cleared the works zones as agreed?
-
Who is the analyst? Is it the same as that detailed in the Method Statement?
-
What is the air monitoring required on the project?
-
Is it any different to that detailed in the Method Statemen
-
Additional Comments - (report here any items required to be rectified from the above and issues reported by the Supervisor / Foreman
-
Contract Manager Supervisor's Name / Date / Signature
Enforcing Authority Visit Form
-
Date / Time:
-
Site Address:
-
Supervisor:
-
Contracts Manager:
-
Enforcing Authority:
-
HSE / Local Area EHO
-
Name of Enforcing Inspector:
-
Contact Details:
-
Findings:
-
Actions:
-
By Whom:
-
Signature of Supervisor:
-
Signature of Enforcing Inspector:
-
This record must be completed on site by the Foreman / Supervisor at the time of the visit. The HSE / EHO may be requested to fill in the form but is not obliged to do so.
Should an officer leave an Instant Visit Report e.g. a FODIR, the form will not be required but the actions below are still required.
ACTIONS:
Should the officer have any concerns the CHSCD Manager and Contracts Manager must be informed verbally as soon as practicable. The form MUST be completed regardless. Failure to do so may result in performance bonus payment being withdrawn.
If it hasn't been recorded, it hasn't happened.
Returm any forms to Contract Manager with THREE days of visit.
Regional Office to send forms to the Corporate Health and Safety Compliance Manager with FIVE days of visit.
AMS01 - Amendments to Method Statement Sheet
-
THIS MUST BE VERBALLY AUTHORISED BY THE CONTRACT MANAGER -
Site Address:
-
Project No:
-
Amendment Number:
-
Date:
-
Reason for Amendment:
-
Any amendments to the plan of work will be made in line with Company Standard Procedure No# O/02 -
Person Amending:
-
Amendments:
-
Authority
-
Name / Position / Signature:
Smoke Test Certification
-
AREA 1 -
This section certifies that the enclosure was effective at retaining the test smoke released. In addition the negative pressure units were effective at clearing the internal atmosphere within 7 minutes, achieving a ratio of a minimum of 8 air changes per hour. Independent Witnesses must be sought wherever possible. Please indicate status below.
-
Name:
-
Independent:
-
Company:
-
Signature:
-
AREA 2 -
This section certifies that the enclosure was effective at retaining the test smoke released. In addition the negative pressure units were effective at clearing the internal atmosphere within 7 minutes, achieving a ratio of a minimum of 8 air changes per hour. Independent Witnesses must be sought wherever possible. Please indicate status below.
-
Name:
-
Independent:
-
Company:
-
Signature:
-
AREA 3 -
This section certifies that the enclosure was effective at retaining the test smoke released. In addition the negative pressure units were effective at clearing the internal atmosphere within 7 minutes, achieving a ratio of a minimum of 8 air changes per hour. Independent Witnesses must be sought wherever possible. Please indicate status below.
-
Name:
-
Independent:
-
Company:
-
Signature:
-
AREA 4 -
This section certifies that the enclosure was effective at retaining the test smoke released. In addition the negative pressure units were effective at clearing the internal atmosphere within 7 minutes, achieving a ratio of a minimum of 8 air changes per hour. Independent Witnesses must be sought wherever possible. Please indicate status below.
-
Name:
-
Independent:
-
Company:
-
Signature:
-
AREA 5 -
This section certifies that the enclosure was effective at retaining the test smoke released. In addition the negative pressure units were effective at clearing the internal atmosphere within 7 minutes, achieving a ratio of a minimum of 8 air changes per hour. Independent Witnesses must be sought wherever possible. Please indicate status below.
-
Name:
-
Independent:
-
Company:
-
Signature:
Day 1 Site Diary
-
MUST BE COMPLETED EVERY DAY
-
Date:
-
Section 1 - Weather -
Section 2 - Operatives Name -
1.
-
2.
-
3.
-
4.
-
5.
-
6.
-
7.
-
8.
-
9.
-
10.
-
11,
-
12.
-
13.
-
14.
-
15.
-
Section 3 - Site Visitors -
Analytical Company:
-
Sub-contractors:
-
Sub - contractors:
-
Safety Manager:
-
Site Safety Auditor:
-
Others (detail):
-
Section 4 - Site Deliveries / Colections -
1. Hire plant / Skips , Company , Signature of Driver:
-
2. Hire plant / Skips , Company , Signature of Driver:
-
3. Hire plant / Skips , Company , Signature of Driver:
-
4. Hire plant / Skips , Company , Signature of Driver:
-
5. Hire plant / Skips , Company , Signature of Driver:
-
Section 5 - Record of Day's Events / Actions Taken - (problems, variations, instructions, delays, hold ups, etc.) -
Date / Time:
-
Events / Actions Taken:
-
Section 6 -
Signature:
Day 2 Site Diary
-
MUST BE COMPLETED EVERY DAY
-
Date:
-
Section 1 - Weather -
Section 2 - Operatives Name -
1.
-
2.
-
3.
-
4.
-
5.
-
6.
-
7.
-
8.
-
9.
-
10.
-
11,
-
12.
-
13.
-
14.
-
15.
-
Section 3 - Site Visitors -
Analytical Company:
-
Sub-contractors:
-
Sub - contractors:
-
Safety Manager:
-
Site Safety Auditor:
-
Others (detail):
-
Section 4 - Site Deliveries / Colections -
1. Hire plant / Skips , Company , Signature of Driver:
-
2. Hire plant / Skips , Company , Signature of Driver:
-
3. Hire plant / Skips , Company , Signature of Driver:
-
4. Hire plant / Skips , Company , Signature of Driver:
-
5. Hire plant / Skips , Company , Signature of Driver:
-
Section 5 - Record of Day's Events / Actions Taken - (problems, variations, instructions, delays, hold ups, etc.) -
Date / Time:
-
Events / Actions Taken:
-
Section 6 -
Signature:
Day 3 Site Diary
-
MUST BE COMPLETED EVERY DAY
-
Date:
-
Section 1 - Weather -
Section 2 - Operatives Name -
1.
-
2.
-
3.
-
4.
-
5.
-
6.
-
7.
-
8.
-
9.
-
10.
-
11,
-
12.
-
13.
-
14.
-
15.
-
Section 3 - Site Visitors -
Analytical Company:
-
Sub-contractors:
-
Sub - contractors:
-
Safety Manager:
-
Site Safety Auditor:
-
Others (detail):
-
Section 4 - Site Deliveries / Colections -
1. Hire plant / Skips , Company , Signature of Driver:
-
2. Hire plant / Skips , Company , Signature of Driver:
-
3. Hire plant / Skips , Company , Signature of Driver:
-
4. Hire plant / Skips , Company , Signature of Driver:
-
5. Hire plant / Skips , Company , Signature of Driver:
-
Section 5 - Record of Day's Events / Actions Taken - (problems, variations, instructions, delays, hold ups, etc.) -
Date / Time:
-
Events / Actions Taken:
-
Section 6 -
Signature:
Day 4 Site Diary
-
MUST BE COMPLETED EVERY DAY
-
Date:
-
Section 1 - Weather -
Section 2 - Operatives Name -
1.
-
2.
-
3.
-
4.
-
5.
-
6.
-
7.
-
8.
-
9.
-
10.
-
11,
-
12.
-
13.
-
14.
-
15.
-
Section 3 - Site Visitors -
Analytical Company:
-
Sub-contractors:
-
Sub - contractors:
-
Safety Manager:
-
Site Safety Auditor:
-
Others (detail):
-
Section 4 - Site Deliveries / Colections -
1. Hire plant / Skips , Company , Signature of Driver:
-
2. Hire plant / Skips , Company , Signature of Driver:
-
3. Hire plant / Skips , Company , Signature of Driver:
-
4. Hire plant / Skips , Company , Signature of Driver:
-
5. Hire plant / Skips , Company , Signature of Driver:
-
Section 5 - Record of Day's Events / Actions Taken - (problems, variations, instructions, delays, hold ups, etc.) -
Date / Time:
-
Events / Actions Taken:
-
Section 6 -
Signature:
Day 5 Site Diary
-
MUST BE COMPLETED EVERY DAY
-
Date:
-
Section 1 - Weather -
Section 2 - Operatives Name -
1.
-
2.
-
3.
-
4.
-
5.
-
6.
-
7.
-
8.
-
9.
-
10.
-
11,
-
12.
-
13.
-
14.
-
15.
-
Section 3 - Site Visitors -
Analytical Company:
-
Sub-contractors:
-
Sub - contractors:
-
Safety Manager:
-
Site Safety Auditor:
-
Others (detail):
-
Section 4 - Site Deliveries / Colections -
1. Hire plant / Skips , Company , Signature of Driver:
-
2. Hire plant / Skips , Company , Signature of Driver:
-
3. Hire plant / Skips , Company , Signature of Driver:
-
4. Hire plant / Skips , Company , Signature of Driver:
-
5. Hire plant / Skips , Company , Signature of Driver:
-
Section 5 - Record of Day's Events / Actions Taken - (problems, variations, instructions, delays, hold ups, etc.) -
Date / Time:
-
Events / Actions Taken:
-
Section 6 -
Signature:
Day 6 Site Diary
-
MUST BE COMPLETED EVERY DAY
-
Date:
-
Section 1 - Weather -
Section 2 - Operatives Name -
1.
-
2.
-
3.
-
4.
-
5.
-
6.
-
7.
-
8.
-
9.
-
10.
-
11,
-
12.
-
13.
-
14.
-
15.
-
Section 3 - Site Visitors -
Analytical Company:
-
Sub-contractors:
-
Sub - contractors:
-
Safety Manager:
-
Site Safety Auditor:
-
Others (detail):
-
Section 4 - Site Deliveries / Colections -
1. Hire plant / Skips , Company , Signature of Driver:
-
2. Hire plant / Skips , Company , Signature of Driver:
-
3. Hire plant / Skips , Company , Signature of Driver:
-
4. Hire plant / Skips , Company , Signature of Driver:
-
5. Hire plant / Skips , Company , Signature of Driver:
-
Section 5 - Record of Day's Events / Actions Taken - (problems, variations, instructions, delays, hold ups, etc.) -
Date / Time:
-
Events / Actions Taken:
-
Section 6 -
Signature:
Day 7 Site Diary
-
MUST BE COMPLETED EVERY DAY
-
Date:
-
Section 1 - Weather -
Section 2 - Operatives Name -
1.
-
2.
-
3.
-
4.
-
5.
-
6.
-
7.
-
8.
-
9.
-
10.
-
11,
-
12.
-
13.
-
14.
-
15.
-
Section 3 - Site Visitors -
Analytical Company:
-
Sub-contractors:
-
Sub - contractors:
-
Safety Manager:
-
Site Safety Auditor:
-
Others (detail):
-
Section 4 - Site Deliveries / Colections -
1. Hire plant / Skips , Company , Signature of Driver:
-
2. Hire plant / Skips , Company , Signature of Driver:
-
3. Hire plant / Skips , Company , Signature of Driver:
-
4. Hire plant / Skips , Company , Signature of Driver:
-
5. Hire plant / Skips , Company , Signature of Driver:
-
Section 5 - Record of Day's Events / Actions Taken - (problems, variations, instructions, delays, hold ups, etc.) -
Date / Time:
-
Events / Actions Taken:
-
Section 6 -
Signature:
DCU Setup Record
-
-
Date / Time:
-
Please tick to confirm the item has been checked:
- Clean
- Sited Level
- Waste Removed
- Circuit Breaker
- Waste water connected to drain
- Water supply connected
- Boiler functioning
- NPU functioning
- Soap / towels / Nail Brush / Gel
- Self - closing doors
- Mirror in place
- Signs in place
- Clearance certificate displayed
-
Faults identified
-
All faults fixed?
-
Signed
-
-
Date / Time:
-
Please tick to confirm the item has been checked:
- Clean
- Sited Level
- Waste Removed
- Circuit Breaker
- Waste water connected to drain
- Water supply connected
- Boiler functioning
- NPU functioning
- Soap / towels / Nail Brush / Gel
- Self - closing doors
- Mirror in place
- Signs in place
- Clearance certificate displayed
-
Faults identified
-
All faults fixed?
-
Signed
-
-
Date / Time:
-
Please tick to confirm the item has been checked:
- Clean
- Sited Level
- Waste Removed
- Circuit Breaker
- Waste water connected to drain
- Water supply connected
- Boiler functioning
- NPU functioning
- Soap / towels / Nail Brush / Gel
- Self - closing doors
- Mirror in place
- Signs in place
- Clearance certificate displayed
-
Faults identified
-
All faults fixed?
-
Signed
-
-
Date / Time:
-
Please tick to confirm the item has been checked:
- Clean
- Sited Level
- Waste Removed
- Circuit Breaker
- Waste water connected to drain
- Water supply connected
- Boiler functioning
- NPU functioning
- Soap / towels / Nail Brush / Gel
- Self - closing doors
- Mirror in place
- Signs in place
- Clearance certificate displayed
-
Faults identified
-
All faults fixed?
-
Signed
-
-
Date / Time:
-
Please tick to confirm the item has been checked:
- Clean
- Sited Level
- Waste Removed
- Circuit Breaker
- Waste water connected to drain
- Water supply connected
- Boiler functioning
- NPU functioning
- Soap / towels / Nail Brush / Gel
- Self - closing doors
- Mirror in place
- Signs in place
- Clearance certificate displayed
-
Faults identified
-
All faults fixed?
-
Signed
-
-
Date / Time:
-
Please tick to confirm the item has been checked:
- Clean
- Sited Level
- Waste Removed
- Circuit Breaker
- Waste water connected to drain
- Water supply connected
- Boiler functioning
- NPU functioning
- Soap / towels / Nail Brush / Gel
- Self - closing doors
- Mirror in place
- Signs in place
- Clearance certificate displayed
-
Faults identified
-
All faults fixed?
-
Signed
-
-
Date / Time:
-
Please tick to confirm the item has been checked:
- Clean
- Sited Level
- Waste Removed
- Circuit Breaker
- Waste water connected to drain
- Water supply connected
- Boiler functioning
- NPU functioning
- Soap / towels / Nail Brush / Gel
- Self - closing doors
- Mirror in place
- Signs in place
- Clearance certificate displayed
-
Faults identified
-
All faults fixed?
-
Signed
-
-
Date / Time:
-
Please tick to confirm the item has been checked:
- Clean
- Sited Level
- Waste Removed
- Circuit Breaker
- Waste water connected to drain
- Water supply connected
- Boiler functioning
- NPU functioning
- Soap / towels / Nail Brush / Gel
- Self - closing doors
- Mirror in place
- Signs in place
- Clearance certificate displayed
-
Faults identified
-
All faults fixed?
-
Signed
-
If a fault has been discovered and cannot be fixed; stop the work seal the DCU and tell the managing director
Half Mask - Weekly Inspection Record
-
Please request more inspection sheets if there are three or more operatives on site and the job is to last longer than ten days. -
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Mask Integrity
- Strap Condition
- Valves
- Cleanliness
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Mask Integrity
- Strap Condition
- Valves
- Cleanliness
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Mask Integrity
- Strap Condition
- Valves
- Cleanliness
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Mask Integrity
- Strap Condition
- Valves
- Cleanliness
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Mask Integrity
- Strap Condition
- Valves
- Cleanliness
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Mask Integrity
- Strap Condition
- Valves
- Cleanliness
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Mask Integrity
- Strap Condition
- Valves
- Cleanliness
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Mask Integrity
- Strap Condition
- Valves
- Cleanliness
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Mask Integrity
- Strap Condition
- Valves
- Cleanliness
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Mask Integrity
- Strap Condition
- Valves
- Cleanliness
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Mask Integrity
- Strap Condition
- Valves
- Cleanliness
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Mask Integrity
- Strap Condition
- Valves
- Cleanliness
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
Full Face Mask - Weekly Inspection Record
-
Please request more inspection sheets if there are three or more operatives on site and the job is to last longer than ten days. -
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Flow Rate
- Exhalation Valve
- Battery Harness
- Battery
- Battery Charge
- Battery Lead
- Head Straps
- Face Piece Visor
- Valves
- Motor
- Face Fit
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Flow Rate
- Exhalation Valve
- Battery Harness
- Battery
- Battery Charge
- Battery Lead
- Head Straps
- Face Piece Visor
- Valves
- Motor
- Face Fit
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Flow Rate
- Exhalation Valve
- Battery Harness
- Battery
- Battery Charge
- Battery Lead
- Head Straps
- Face Piece Visor
- Valves
- Motor
- Face Fit
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Flow Rate
- Exhalation Valve
- Battery Harness
- Battery
- Battery Charge
- Battery Lead
- Head Straps
- Face Piece Visor
- Valves
- Motor
- Face Fit
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Flow Rate
- Exhalation Valve
- Battery Harness
- Battery
- Battery Charge
- Battery Lead
- Head Straps
- Face Piece Visor
- Valves
- Motor
- Face Fit
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Flow Rate
- Exhalation Valve
- Battery Harness
- Battery
- Battery Charge
- Battery Lead
- Head Straps
- Face Piece Visor
- Valves
- Motor
- Face Fit
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Flow Rate
- Exhalation Valve
- Battery Harness
- Battery
- Battery Charge
- Battery Lead
- Head Straps
- Face Piece Visor
- Valves
- Motor
- Face Fit
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Flow Rate
- Exhalation Valve
- Battery Harness
- Battery
- Battery Charge
- Battery Lead
- Head Straps
- Face Piece Visor
- Valves
- Motor
- Face Fit
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Flow Rate
- Exhalation Valve
- Battery Harness
- Battery
- Battery Charge
- Battery Lead
- Head Straps
- Face Piece Visor
- Valves
- Motor
- Face Fit
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Flow Rate
- Exhalation Valve
- Battery Harness
- Battery
- Battery Charge
- Battery Lead
- Head Straps
- Face Piece Visor
- Valves
- Motor
- Face Fit
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Flow Rate
- Exhalation Valve
- Battery Harness
- Battery
- Battery Charge
- Battery Lead
- Head Straps
- Face Piece Visor
- Valves
- Motor
- Face Fit
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
-
-
Name:
-
Date:
-
Please tick to confirm item has been checked
- Flow Rate
- Exhalation Valve
- Battery Harness
- Battery
- Battery Charge
- Battery Lead
- Head Straps
- Face Piece Visor
- Valves
- Motor
- Face Fit
-
Identification Tag Number
-
Faults identified
-
Fit for use?
-
Signed
Decontamination Units
-
Please ensure checklist is completed at pick up.
Keep doors locked and take out keys.
Make sure DCU is totally clean; do not rely on it having an air test.
Report any defects. -
Unit in Use
-
Site Address:
-
Unit Identification No:
-
Date delivered / Collected:
-
Date removed / returned
-
Site Supervisor:
-
Week Commencing Date standards checked:
-
Please tick the days each standard was checked
-
Air Test Certificate
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Cleanliness
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Internal Lights OK
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
No. Ext. Damage
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Keys Available
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
On Level Ground
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Steps
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
LPG Cylinder OK
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Water Heated OK
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Water Filters in Use
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Drain to Foul
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
240v Power Lead
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Earthing Rod in Use
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Lockers OK
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Heating OK
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Shower Drains OK
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Shower Heads OK
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Shower Caps Present
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
SC Doors Operate
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
HEPA Filter ON NPU
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Nail Brush
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Mirror
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Towels
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Mop / Bucket
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Waste Bags
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Transit Route Short
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Carbon Monoxide Detector Working
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
Inspection of Enclosure and Airlocks
-
-
WEEKLY RECORD OF TWICE DAILY INSPECTION
Following items of the enclosure must be inspected an confirmed on a twice daily basis.
Please indicate time in the appropriate column. Two entries per day are required.
Where the items fail the inspection, immediate remedial measures must be actioned and completed before work commences / recommences. -
Day 1 -
Date:
-
Time of First inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Time of Second inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Name and Signature
-
Day 2 -
Date:
-
Time of First inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Time of Second inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Name and Signature
-
Day 3 -
Date:
-
Time of First inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Time of Second inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Name and Signature
-
Day 4 -
Date:
-
Time of First inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Time of Second inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Name and Signature
-
Day 5 -
Date:
-
Time of First inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Time of Second inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Name and Signature
-
Day 6 -
Date:
-
Time of First inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Time of Second inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Name and Signature
-
Day 7 -
Date:
-
Time of First inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Time of Second inpection
-
Please detail items checked:
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Name and Signature
Inspection of Vacuum Equipment
-
WEEKLY RECORD OF DAILY INSPECTION
The following items must be inspected and confirmed on a daily basis. Please indicate the days each item were checked. -
Negative Pressure Units -
Serial No. S:
-
Re-test Dates:
-
Inspection Week Commencing Date
-
Numbers correspond with numbers stated in Plan of Work
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Appropriate DOP certs available
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Hose and unit in good repair
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Located Farthest end from airlocks venting to outside where possible
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Filter changed daily
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Name and Signature:
-
'H' Type Vacuum Units -
Serial No. S:
-
Re-test Dates:
-
Inspection Week Commencing Date
-
At least 2 units available on site (one at dirty end of airlock for decontamination)
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Appropriate DOP certs available
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Hose & Unit in good repair
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Hepa Filter installed
- Monday
- Tuesday
- Wednesday
- Thursday
- Friday
- Saturday
- Sunday
-
Is any remedial action required?<br>If yes please detail action required , by whom and the time frame given
-
Name and Signature:
Ladders Weekly Inspection and Pre-Use Checklist
-
The condition of step ladders must be inspected and recorded by users prior to use.
Defective Equipment MUST NOT be used. Risk Assessment must be in place. -
Type of Ladder:
-
Ref / Identification Number:
-
User Name and Signature:
-
Inspection Date:
-
Please include details of any faults or defects
-
Front & Rear Sections -
Stiles - twisted or distorted
-
Treads - cracked, split
-
Treads loose - considered loose if moved by hand
-
Bottom diagonals - twisted or distorted
-
Bottom diagonals - loose or missing
-
Rubber feet - damaged, worn or missing
-
Rivets etc. - loose or missing
-
Rear Section Only -
Leg angles - cracked, split, worn or broken
-
Leg angles - twisted or distorted
-
Cross angles - cracked, split, worn or broken
-
Cross angles - twisted or distorted
-
Top hinge - worn or broken
-
Side stabilisers - twisted or distorted (where fitted)
-
Side stabilisers - worn or broken (where fitted)
-
-
Is a ladder, step ladder, etc. the right equipment for the work?
-
If so, is the equipment in good condition and free from slippery substances?
-
Can the leaning ladder be secured at the bottom?
-
If not, can it be secured at the bottom?
-
If not, will a second person stationed at the base provide sufficient safety?
-
Is the top rung level with the platform?
-
Is there adequate handhold at the place of landing?
-
Are there platforms at 9m maximum intervals?
-
Is the ladder angle correct (1:4)?
-
Is the support for the ladder adequate at both the upper point of rest and the foot?
-
Is the ladder properly positioned?
-
If it is necessary to carry tools of equipment, has provision been made to allow for here point contact climbing - use of tool belts, hauling etc.?
-
If an extension ladder is used, is there sufficient overlap between sections?
-
On the step ladders are they stays, chains or cords in good condition?
-
Can the ladder be placed sufficiently near the work on a firm level surface?
-
Is the ladder clear of overhead electric cables?
Mobile Scaffold Weekly Inspection and Pre Use Checklist
-
Check Sheet: Issue, Use and Return
-
The condition of the Mobile Tower Scaffold must be inspected and recorded by users prior to use.
Defective Equipment MUST NOT be used. Risk Assessment must be in place. -
Type of Tower Scaffold:
-
Ref / Identification Number
-
By Whom:
-
Date:
-
MPL:
-
Signature:
-
Have competent persons been in charge of erection / installation?
-
Is a copy of the manufacturer's assembly instructions available?
-
Have all component parts and boards been visually examined and are free from defects?
-
Are the castors of suitable size with effective locking devices?
-
Do the castors roll freely and lock securely?
-
Is the maximum permitted load (MPL) of the scaffold known? Indicate above.
-
Has the MPL been communicated to all users / potential users?
-
Is the ground location capable of taking the combined weight of the scaffold and its loading?
-
Is the tower level and plumb?
-
Is the tower height less than 4 times the minimum base width (unless manufacturer's instructions indicate otherwise)?
-
Is the tower fully braced on all sides?
-
Have stabilisers or outriggers been fixed to the tower?
-
Are the stabilisers / outriggers in firm contact with the ground?
-
Are the stabilisers / outriggers at full spread to maximise stability?
-
Are the guardrails and toe-boards installed and secures? (Absolute requirement at working platform heights greater than 1.2m)
-
Is the working platform board correctly located with the access hatch adjacent to the internal ladders or staircase?
-
Has the tower scaffold been erected at safe distance from overhead cables (<4m)?
-
If the tower is to be left incomplete, has a sign been displayed warning that it is unsafe to climb?
-
Has the surrounding area been cordoned off?
-
If extra stability is necessary can the tower scaffold be tied to a neighbouring structure?
-
If you have answered 'NO' to any of the above - DO NOT USE.
Completion of Works Declaration
-
This form is applicable to all Certificate of reoccupation works.
All declarations below must be completed and signed by the site supervisory staff working on behalf of Delta Services. The actions must be completed by the appointed site supervisor / foreman only. The responsibility for these actions must not be delegated to an operative.
Failure to comply may result in disciplinary action. -
Site Address:
-
Job No:
-
Enclosure / Work Area:
-
Analytical Company:
-
Part 1. Inspection Inside Enclosure / Work Area (Pre - analyst Visual Inspection)
-
I have completed a thorough visual examination around and within the enclosure / work area prior to inspection by an independent analyst. I can confirm that the works detailed in the Plan of Works have been completed, that the area meets satisfactory levels of cleanliness with safe and suitable means of access and egress throughout the enclosure / work area to allow a Certificate of Reoccupation (COR) Stage 2 visual inspection by the visual analyst.
-
Signature:
-
Name:
-
Part 2. COR Stage 1,2&3 Visual Inspection and Clearance Air Sampling.
-
I have accompanied the analyst during COR stage 1 preliminary & stage 2 visual inspection and have ensured that any required remedial actions have completed to their satisfaction prior to COR stage 3 Clearance Air Sampling.
-
Signature:
-
Name:
-
Time and Date:
-
Time and Date:
-
Part 3. COR Stage 1,2&3 Visual Inspection and Clearance Air Sampling.
-
I have accompanied the analyst during inspection of the area within and around the dismantled enclosure / work area. The areas are free of asbestos debris and enclosure materials with the exception of materials required to maintain segregation of adjacent asbestos-contaminated areas as identified in the Plan of Work and the COR.
The hygiene unit is dry, free of visible dust, debris and waste, has passed a disturbance air test and is suitable for subsequent use or return to hirer. Certificate of Reoccupation and Hygiene Facility clearance certificate has / will be issue. -
Signature:
-
Name:
-
Time and Date:
-
Part 4. Final Assessment
-
Visible dust and debris to plant and equipment from within the work area has been removed, or contaminated equipment has been sealed and labelled prior to removal form the site or transfer to the next work area. Equipment on hire is clean and fit for return to hirer or transfer to next work area. all waste has been removed / is securely stored in a suitable container awaiting removal. The site / work area has been left in a clean and tidy condition.
-
Signature:
-
Name:
-
Time and Date:
-
N.B. Disciplinary action may be a possible outcome for any signatory who has failed to complete the processes and the document with full integrity. this will include the failure to personally complete the physical examination required or making a statement known or proven to be untrue, this is not an exhaustive list of potential causes of disciplinary action.
Site Inspection & Examination
-
Site Details
-
Manager:
-
Supervisor / Foreman:
-
Office:
-
Job Number:
-
Site Address:
-
Type of Asbestos:
-
Was the project notified? if yes please give the date when
-
Observation and Summary:
-
Date:
-
Visual Examination of Enclosure (tick description of activities at time of inspection)
-
Please tick applicable
- Works in Progress
- Following Pre-visual by Supervisor
- Following Visual by Analyst
- Following Site Clearance
-
Description of findings & action(s) required:
-
Analyst on site:
-
Analytical Company:
-
Site Evaluation -
Site Documentation
-
Are there copies on site of the asbestos license and employers liability insurance certificate?
-
Are there copies of the ASBS, Method of Work (with sketch plan) and the Company standard procedures on site?
-
Has the method of Work and sketch plan been amended to reflect the actual site workings?
-
Is there an up to date site diary available including all inspection sheets (DCU, Enclosures, Vacuum and NPU, etc.)?
-
Is there a current set of risk and CoSHH assessments on site?
-
Has all air monitoring (as per the Method of Work) been booked and carried out?
-
Enclosure / Airlocks -
Are the smoke test records available for inspection and independently witnessed?
-
Is the enclosure in sound condition to prevent the spread of asbestos, adequately illuminated and has vision panels / CCTV available for external viewing?
-
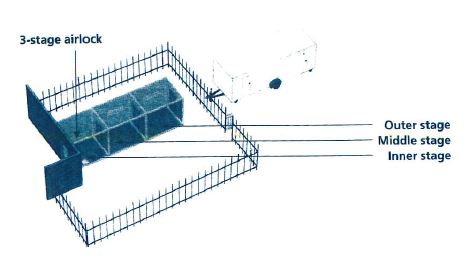
Are correct warning signs displayed and does the airlock consist of 4 cubes 1m2 x 2m (minimum 1 vision panel in dirty end) with flaps weightened and hanging on enclosure side?
-
Plant on Site
-
Is there sufficient equipment in place to ensure partial negative pressure, at a point as far away from the airlock as possible and being vented to an outside atmosphere (where practical)?
-
Are there at least 2 H-type vacuums on site (including 1 adjacent to or in the dirty end of the airlock) for preliminary decontamination?
-
Are the DOP test certificates for all plant in date and is plant in suitable condition?
-
Hygiene Facility
-
Is the DCU / MSDU attached / unattached as per the Method of Work and fully operational (water, electric, etc.)?
-
Is the unit level, clean and are there adequate numbers of shower heads (1 per every 4 operatives) with a heated water supply?
-
Is the transit route as short as possible, signed (protected) and away from occupied areas?
-
Site organisation/ Method of Work – Has all non-contaminated loose equipment and material been removed from the work area?
-
Has all non-contaminated foxed plant, etc. been vacuum cleaned, covered and sealed?
-
Is the Method of Work stated in the Plan of Work appropriate for the work being carried out?
-
Is the Method of Work being employed on site compliant with that stated in the Plan of Work and suitable for the work being carried out?
-
Is the dust suppression method as that indicated in the Plan of Work, and is it suitable for the task at hand (are hand tools being used whenever possible).?
-
Are the RPE, filter and PPE as those stated in the Method of Work (i.e. suitable) and do all the operatives have their own up-to-date register of training, medical and face fit certificates, etc.)?
-
Waste and Vehicles
-
Are the waste disposal arrangements as those described in the Method of Work (is the consignment note available), is waste double bagged / wrapped, clearly marked, sealed and locked away at all times?
-
Is there a separate bag-lock for waste (if not – why not?) is waste clearly segregated from the other plant and equipment?
-
Is the company vehicle of a suitably clean and tidy standard and free of asbestos debris?
Contact Manager End of Project Evaluation
-
The condition of step ladders must be inspected and recorded by users prior to use.
-
Site Details
-
Contact Manager
-
Supervisor / Foreman
-
Office
-
Job Number
-
Project Site Address
-
Type of Asbestos
-
Was the project notifiable?
-
Overall Project Evaluation by Manager -
Did the project complete on time? And on what date? If not was the HSE notified in writing or delay to project end?
-
Did the project start on the planned date? If not was the HSE notified in writing of delay to start date?
-
Has the plan of work had to be amended> if so were the amendments approved by you.
-
Was the site paperwork returned on time and at least once a weak as appropriate? For example time sheets, exposure records, monitoring sheet etc.
-
Have all consignment notes been completed (one for each movement of waste) and returned to the sit file if not why?
-
Have any complaints / concerns been raised during the project by any of the following: client / neighbour / general public / analyst / auditor / site team? If so what was the complaint / concern and how was it resolved?
-
Was the time keeping and punctuality of the site team acceptable?
-
Did the site team present an acceptable image of Delta Services? (well presented, clean, tidy, uniform worn, respectable attitude)
-
Were any issues / concerns raised during the project in relation to the equipment? For example plant and Machinery, personal protection.
-
Did any type of accidents / incident / near misses occur during this project? How were the issues above resolved?
-
If the above is not applicable, at what pint did you liaise with the site fireman / supervisor or team on site?
-
Was an audit carried out on this project? Were any ‘strikes’ recorded by the auditor? If so, what arrangements/ discussions have you actioned to address the causes of the strike?
-
Have you renewed the visual clearance signing off sheets for this project? If not why?
-
Signature
-
Date