




Title Page
-
Site conducted
-
Notification Number
-
myEHS Event ID
-
Event Type
-
Date
-
Prepared By
-
Location
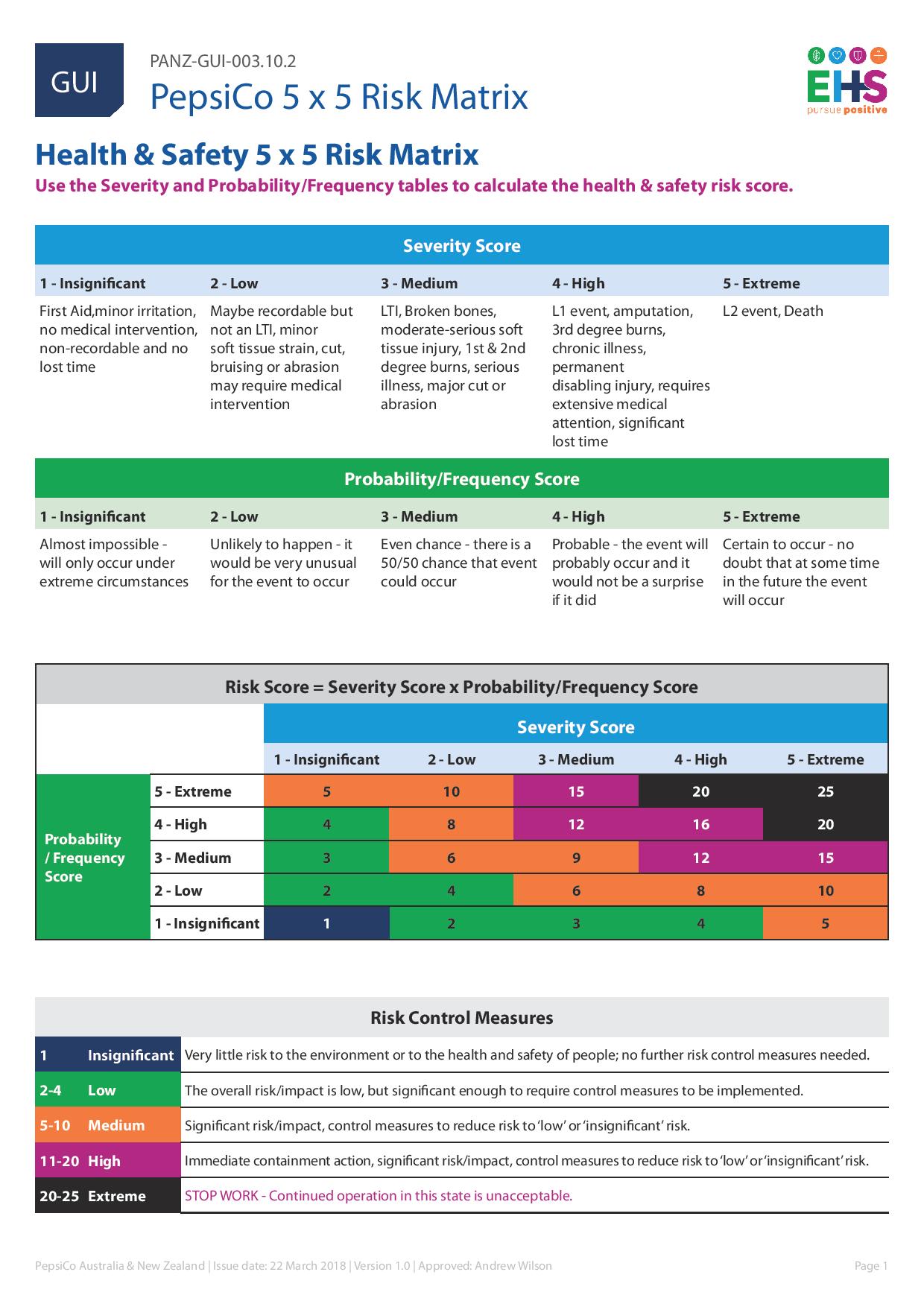
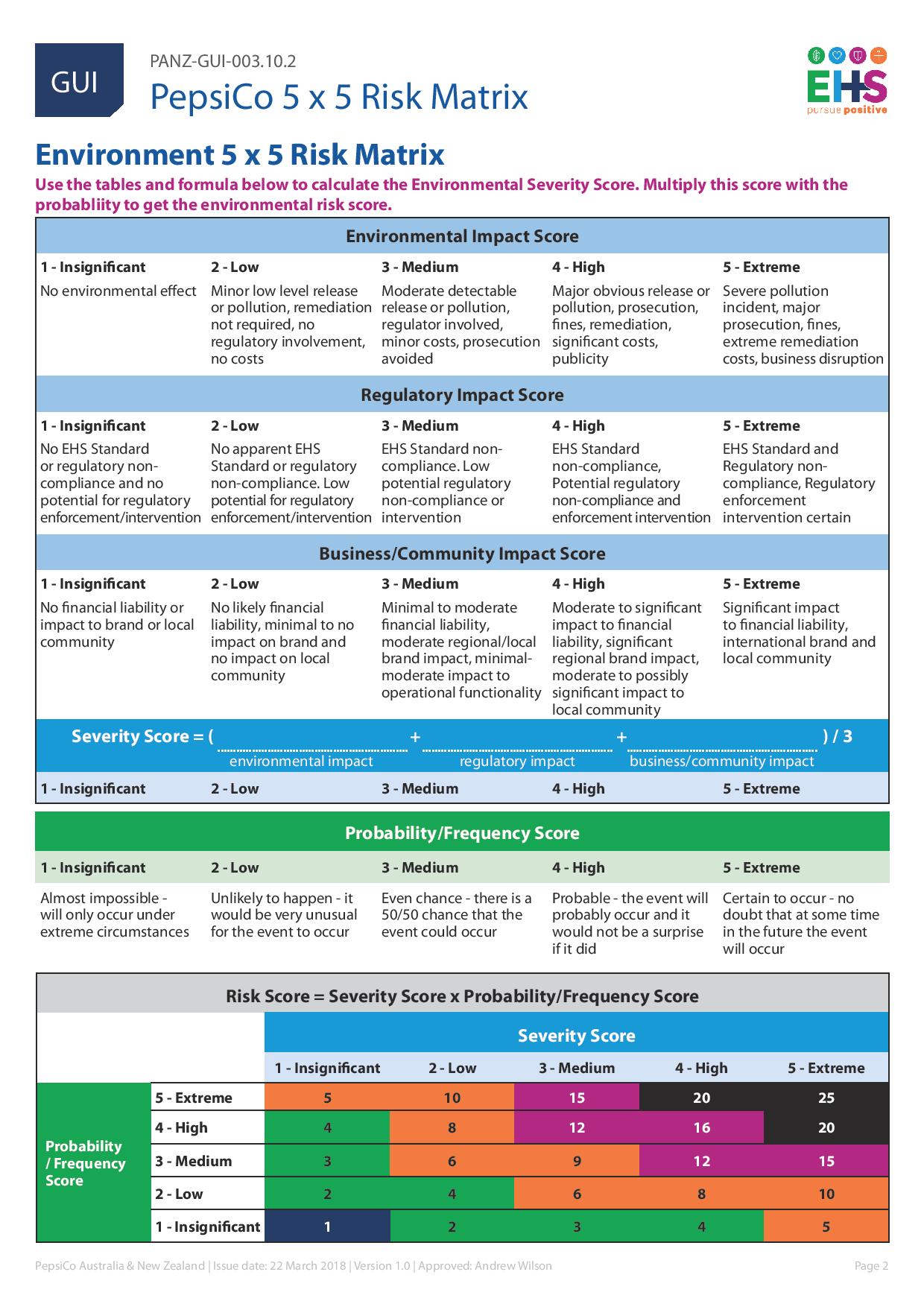
HEALTH AND SAFETY 5X5 RISK MATRIX
-
Please use attached matrix's to calculate the health and safety and Environmental risk scores.
-
A. About the Event - to be completed by the person involved
-
Event Type
-
Incident
-
AOD Checklist to be completed
-
Near Miss hazard
-
AOD Checklist to be completed
-
Inspection
-
General Inquiry / Compliant
-
Event Date & Time
-
Department
-
Specific Area/Location (e.g. line, rego)
-
Event Classification
-
Did this happen at a non-PepsiCo workplace (e.g. supermarket)?
-
Note: If yes You MUST inform the client immediately.
-
Describe what happened/what could have happened/hazard details (include exact location, details of task being undertaken, plant, equipment, substance involved). Attach additional information/form as required.
-
Were there any witnesses?
Witness
-
Name
-
Contact Number
-
Location
-
What have you done to remove or reduce the immediate risk?
-
Work Request Number
B. About the Person Reporting - to be completed by the person involved
-
Person involved
-
Company Name
-
Function
- Ops-Manufacturing
- Ops-S&D
- Transport
- Agro
- Sales
- R&D
- Other (e.g. Admin/HR/IT/Accounts)
-
Specify
-
Family Name
-
Given Name(s)
-
Occupation
-
Person Reporting (If different to person involved)
-
Who have you notified about this event? (You MUST notify a PepsiCo Supervisor within 2 hours & by the end of your shift)
-
What date & time did you notify them?
-
Involved Person Signature
-
Supervisor Signature
C. Impact of the Event - to be completed by the person Supervisor
-
Event Impact
- Real (actual loss/injury)
- Potential (for near miss/hazards)
-
Nature of Impact
-
HUMAN NATURE IMPACT:
-
Work related?
-
Level of Treatment
-
Part of the Body (specify left or right part)
-
Type of Injury (e.g. cut/sprain/bruise etc)
-
Injury treatment conducted?
-
First Aider Name & Sign (if applicable)
-
First Aider Date (if applicable)
-
Treatment Given
-
Injured person returned to work?
-
Date & time the injured person returned to work
-
ENVIRONMENT NATURE IMPACT:
-
Medium Impacted
- Air
- Water
- Waste
- Ground
- Chemical
- Other
-
Specify
-
Location
-
Reportable Quantities Exceeded?
-
DURATION OF THE EVENT:
-
Date & Time Started
-
Date & Time Stopped
-
Type, Volume and Concentration of any substances released (if applicable)
-
Sample Taken?
-
Spill response equipment used/deployed (if applicable)
-
Category of Impact (select the most severe impact level)
- Undetermined
- Near Miss
- Level 0
- Level 1 (immediate escalation required)
- Level 2 (immediate escalation required)
Human Impact
-
Work Related
-
Level of Treatment
-
Part of Body
-
Left/ Right
-
Type of Injury. e.g cut/sprain/bruise etc.
Injury Treatment
-
First Aider name if Applicable
-
First Aider Signature if Applicable
-
First Aider Date (If Applicable)
-
Treatment given if applicable
-
Date injured person returned to work.
-
Time injured person returned to work
-
Not yet returned to work
Environmental
-
Medium Impacted
- Air
- Water
- Waste
- ground
- Chemical
- Other ( please specify)
-
Location
-
Reportable Quantities Exceeded?
-
Duration of Event: Date and Time Started
-
Date and Time Stopped
-
Type , Volume and concentration of any substances released ( If Applicable)
-
Sample Taken
-
Spill response Equipment used/deployed if applicable.
D. Potential Severity - What could have happened - to be completed by the Supervisor
-
Completed in Consultation With : (Name & Signature)
-
Date
-
Consequence
-
Likelihood
-
Outcome
-
Extreme - HIPO (If yes follow correct Escalation Procedure FULL Investigation required)
-
High - HIPO (If yes follow correct Escalation Procedure FULL Investigation required)
-
Moderate Outcome
-
Low Outcome
E. Immediate Causes of the Event - to be completed by the investigation team
-
Completed in Consultation With (minimum required: HSR & Management representative for Near Miss. Refer to investigation procedure for further details)
-
Immediate cause of the incident
-
Details
-
Completion of the investigation including root causes must occur within 14 days & be loaded to myEHS
F. Immediate Corrective Action Taken
-
Immediate Corrective Actions to Prevent Further Loss
Action
-
Description of Action Taken
-
By Who
-
Date of Completion
-
my EHS Action Plan ID Number
G. About the Supervisor Completing this Form
-
Family Name & Given Name(s)
-
Contact Number
-
Occupation
-
Sign
-
Date
H. Circulation
-
Employee (feedback received) : (Name & Signature)
-
Date
-
EHS Management Team : (Name & Signature)
-
Date
undefined
PANZ-FOR-028 AOD REASONABLE SUSPICION ASSESSMENT CHECKLIST
-
Checklist instructions: Where workers are involved in an incident /near miss the Supervisor or Manager must complete the AOD reasonable suspicion checklist as part of the incident reporting process to determine if a worker’s fitness for work may have been a contributing factor in the cause of the incident. If fitness for work factors are identified below refer to PANZ-POL- 004 Alcohol and Other Drugs Policy for further instruction. Where possible and reasonable, observations should be confirmed by another supervisor and/or manager prior to initiating testing.
EMPLOYEES DETAILS
-
Name:
-
Position:
-
Department:
-
Shift:
-
Managers name:
-
Position:
OBSERVATIONS:
-
Supervisor/manager to list observations that are out of character and that lead to safety performance concerns.
SPEECH
-
Slurred
-
Thick
-
Incoherent
-
Shouting
-
Rambling
EYES
-
Bloodshot
-
Glassy
-
Watery
-
Dilated
-
Droopy
APPEARANCE
-
Grinding of teeth
-
Having odour
-
Unusually dishevelled
-
Flushed
-
Pale
-
Sweaty
EXPRESSION
-
Blank
-
Unresponsive
-
Panicked
-
Confused
BEHAVIOUR
-
Agitated
-
Argumentative/Threating
-
Drowsy
-
Stupor-like
-
Hyperactive
-
Unusually Talkative
-
Erratic
-
Dazed
-
Uncommunicative
-
Uncooperative
-
Defiant
-
Emotional/crying
-
Unusually calm
-
Nervous
MOVEMENTS
-
Unsteady/Swaying/Staggering
-
Fumbling/Jerky/Uncoordinated
-
Excessively Slow /Delibrate
-
Excessively Fast / Reckless
-
Shaking/Tremulous
-
Sagging/Leaning
MISCELLANEOUS
-
Presence of alcohol, suspected drugs and/or paraphernalia in possession or in vacinity
-
Admission of possession /usage of alcohol and/or drugs
-
Difficulty in recalling instructions
-
On-the-job misconduct
-
Suspicious and unusual behaviour (please detail below)
-
Changes in work pattersns/performance
OTHER OBSERVATIONS/FURTHER DETAILS (Supervisor/Manager to specify)
-
WHERE AOD TESTING HAS BEEN DEEMED NECESSARY PLEASE CONTACT : INTEGRITY SAMPLING ON PHONE 1800 633 838.
OBSERVATION VERIFICATION (To be completed by the observing supervisor/manager)
-
Date:
-
Time:
-
Signature
CONFIRMATION OF OBSERVATIONS ( To be completed by another supervisor prior to testing)
-
Date:
-
Time:
-
Signature:
COMPLETION OF EVENT NOTIFICATION FORM. (When all information above has been completed please select yes to submit form)
-
When ALL sections have been completed, please select yes to submit.






